

Income Level and Impaired Kidney Function Among Working Adults in Japan
- PMID: 38427342
- PMCID: PMC10907921
- DOI: 10.1001/jamahealthforum.2023.5445
Income Level and Impaired Kidney Function Among Working Adults in Japan
Abstract
Importance: Chronic kidney disease (CKD) is a major public health issue, affecting 850 million people worldwide. Although previous studies have shown the association between socioeconomic status and CKD, little is known about whether this association exists in countries such as Japan where universal health coverage has been mostly achieved.
Objective: To identify any association of income-based disparity with development of impaired kidney function among the working population of Japan.
Design, setting, and participants: This was a nationwide retrospective cohort study of adults aged 34 to 74 years who were enrolled in the Japan Health Insurance Association insurance program, which covers approximately 40% of the working-age population (30 million enrollees) in Japan. Participants whose estimated glomerular filtration rate (eGFR) had been measured at least twice from 2015 to 2022 were included in the analysis, which was conducted from September 1, 2021, to March 31, 2023.
Exposure: Individual income levels (deciles) in the fiscal year 2015.
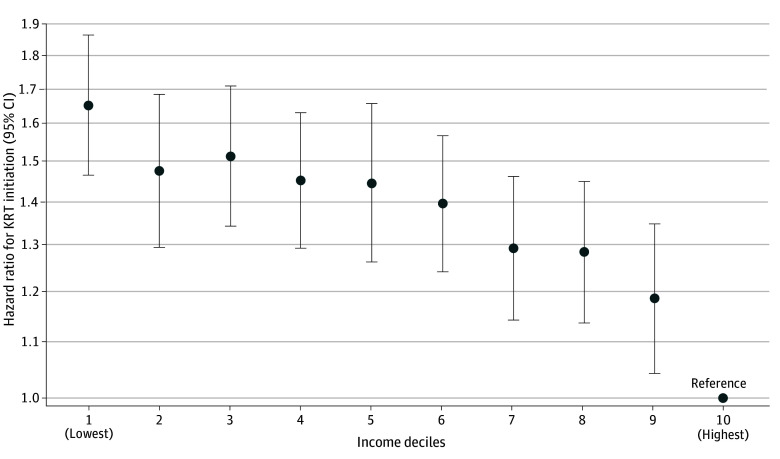
Main outcomes and measures: Odds ratios were calculated for rapid CKD progression (defined as an annual eGFR decline of more than 5 mL/min/1.73 m2), and hazard ratios, for the initiation of kidney replacement therapy (dialysis or kidney transplant) by income level deciles in the fiscal year 2015.
Results: The study population totaled 5 591 060 individuals (mean [SD] age, 49.2 [9.3] years) of whom 33.4% were female. After adjusting for potential confounders, the lowest income decile (lowest 10th percentile) demonstrated a greater risk of rapid CKD progression (adjusted odds ratio, 1.70; 95% CI, 1.67-1.73) and a greater risk of kidney replacement therapy initiation (adjusted hazard ratio, 1.65; 95% CI, 1.47-1.86) compared with the highest income decile (top 10th percentile). A negative monotonic association was more pronounced among males and individuals without diabetes and was observed in individuals with early (CKD stage 1-2) and advanced (CKD stage 3-5) disease.
Conclusions and relevance: The findings of this retrospective cohort study suggest that, even in countries with universal health coverage, there may be a large income-based disparity in the risk of rapid CKD progression and initiation of kidney replacement therapy. These findings highlight the importance of adapting CKD prevention and management strategies according to an individual's socioeconomic status, even when basic health care services are financially guaranteed.
Conflict of interest statement
Figures



References
-
- Foreman KJ, Marquez N, Dolgert A, et al. . Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018;392(10159):2052-2090. doi:10.1016/S0140-6736(18)31694-5 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
