

Awake tracheal intubation in routine airway management: A retrospective analysis in a tertiary centre
- PMID: 38427680
- PMCID: PMC10906896
- DOI: 10.1371/journal.pone.0299071
Awake tracheal intubation in routine airway management: A retrospective analysis in a tertiary centre
Abstract
Introduction: While awake tracheal intubation (ATI) is regarded as the gold standard for difficult airway management according to current guidelines, there seems to be a reluctance in its application. This retrospective cohort study, conducted at a German tertiary hospital over a 2-year period, aimed to demonstrate that integrating awake tracheal intubation using flexible bronchoscopy (ATI:FB) into routine airway management makes it a successful and safe approach.
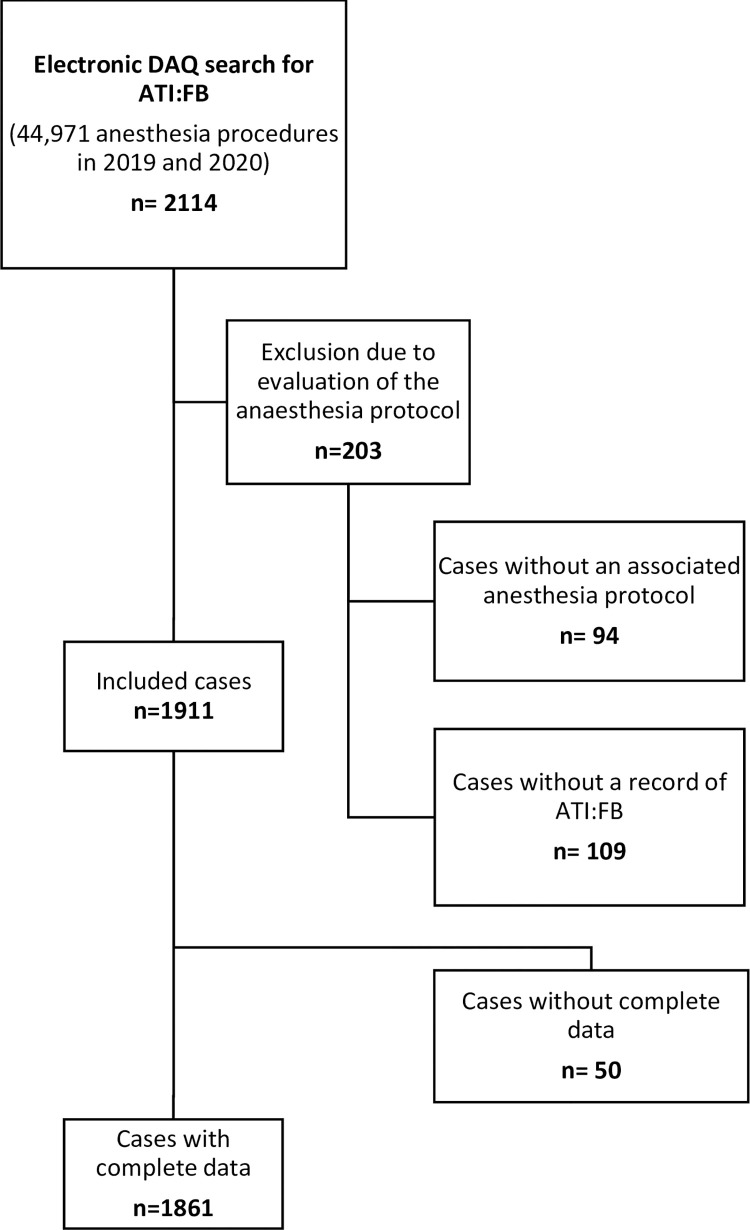
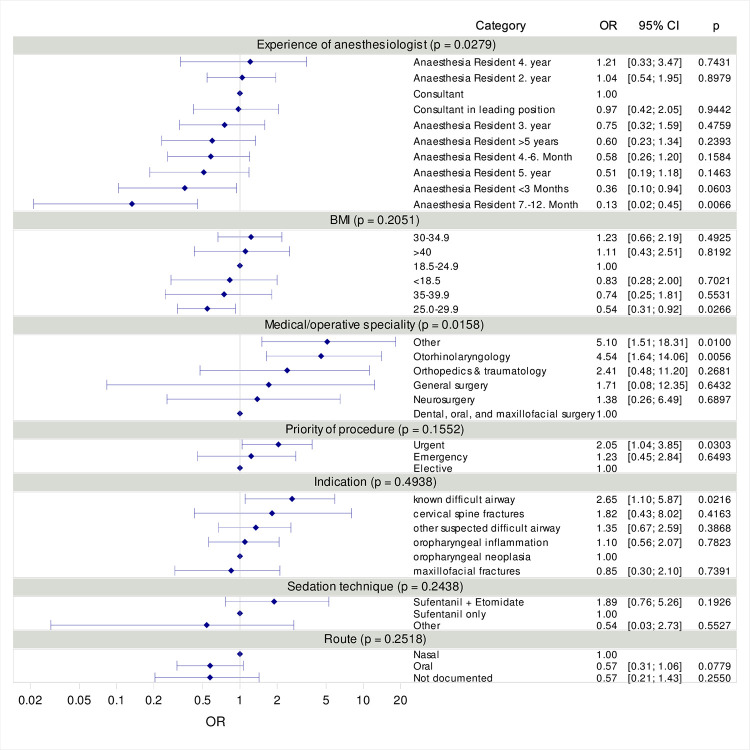
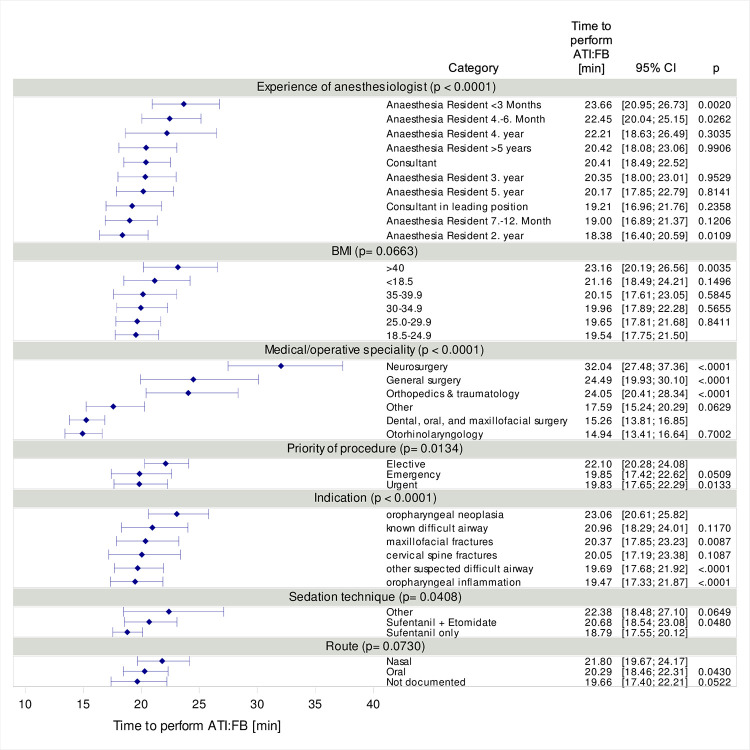
Materials and methods: In 2019 and 2020, records from the data acquisition system (DAQ) and archived anesthesia records were screened to evaluate the specifics of ATI:FB procedures, focusing on overall success and safety. Analysis included complications, time required for ATI:FB, and potential influencing factors such as patient characteristics, indication, medical/operative specialty, sedation technique, route and experience of anesthesiologist. Logistic regression assessed the impact of various variables on occurrence of complications and linear regression, with log(time) as the dependent variable, evaluated median time required to perform ATI:FB.
Results: ATI:FB constituted 4.3 % (n = 1,911) of all airway management procedures, predominantly observed in dental, oral, and maxillofacial surgery (46.5 %) and otorhinolaryngology (38.4 %). The success rate for ATI:FB was notably high at 99.6 %, with only 5.4 % of cases experiencing complications, including technical issues, agitation, and visibility obstruction due to mucous secretion. Complication risk was influenced by the medical specialty and the experience of the anesthesiologist. A strong effect was observed in otorhinolaryngology (OR = 4.54, 95 % CI [1.64; 14.06]). The median time required for ATI:FB was 16 minutes (IQR: 11 to 23), with factors such as indication (p < 0.0001), experience of anesthesiologist (p < 0.0001), sedation technique (p = 0.0408), priority of the procedure (p = 0.0134), and medical/operative specialty (p < 0.0001) affecting the duration. The median time required for ATI:FB differed significantly based on the experience of the anesthesiologist (p < 0.0001).
Conclusion: ATI:FB proves successful and safe, with low complications and manageable procedural time. Experience of the anesthesiologist is a modifiable factor enhancing safety, emphasizing the need for ATI:FB integration into routine airway management.
Copyright: © 2024 Pirlich et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Law JA, Morris IR, Brousseau PA, de la Ronde S, Milne AD. The incidence, success rate, and complications of awake tracheal intubation in 1,554 patients over 12 years: an historical cohort study. Can J Anaesth 2015; 62: 736–44. - PubMed
-
- Joseph TT, Gal JS, DeMaria S Jr., Lin HM, Levine AI, Hyman JB. A Retrospective Study of Success, Failure, and Time Needed to Perform Awake Intubation. Anesthesiology 2016; 125: 105–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
