

Supermicrosurgery lymphaticovenous and lymphaticolymphatic anastomosis: Technical detail and short-term follow-up for immediate lymphatic reconstruction in breast cancer treatment-related lymphedema prevention
- PMID: 38428499
- PMCID: PMC11523392
- DOI: 10.1016/j.jvsv.2024.101863
Supermicrosurgery lymphaticovenous and lymphaticolymphatic anastomosis: Technical detail and short-term follow-up for immediate lymphatic reconstruction in breast cancer treatment-related lymphedema prevention
Abstract
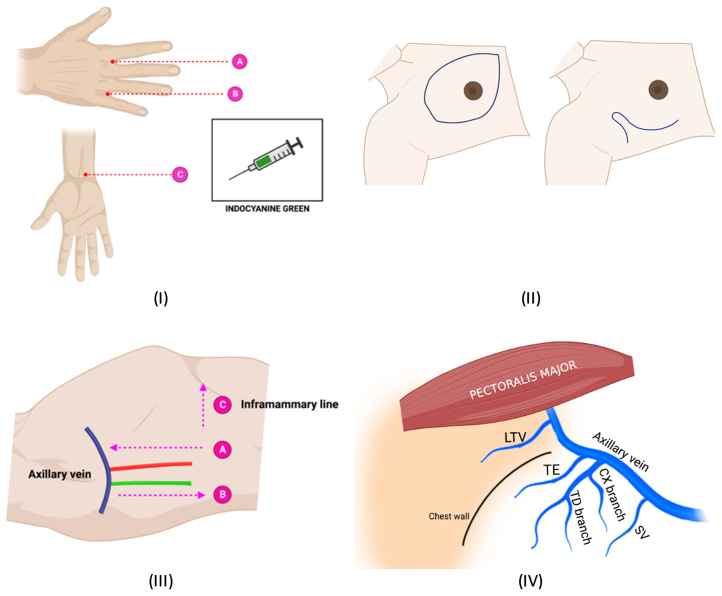
Objective: We describe the feasibility and short-term outcome of our surgical technique to repair the lymph vessel disruption directly after axillary lymph node dissection during breast cancer surgery. This procedure is called immediate lymphatic reconstruction to prevent breast cancer treatment-related lymphedema (BCRL), which frequently occurs after axillary lymph node dissection. The surgical technique consisted of lymphaticovenous anastomosis (LVA) or lymphaticolymphatic anastomosis. We named the procedure lymphatic bypass supermicrosurgery (LBS).
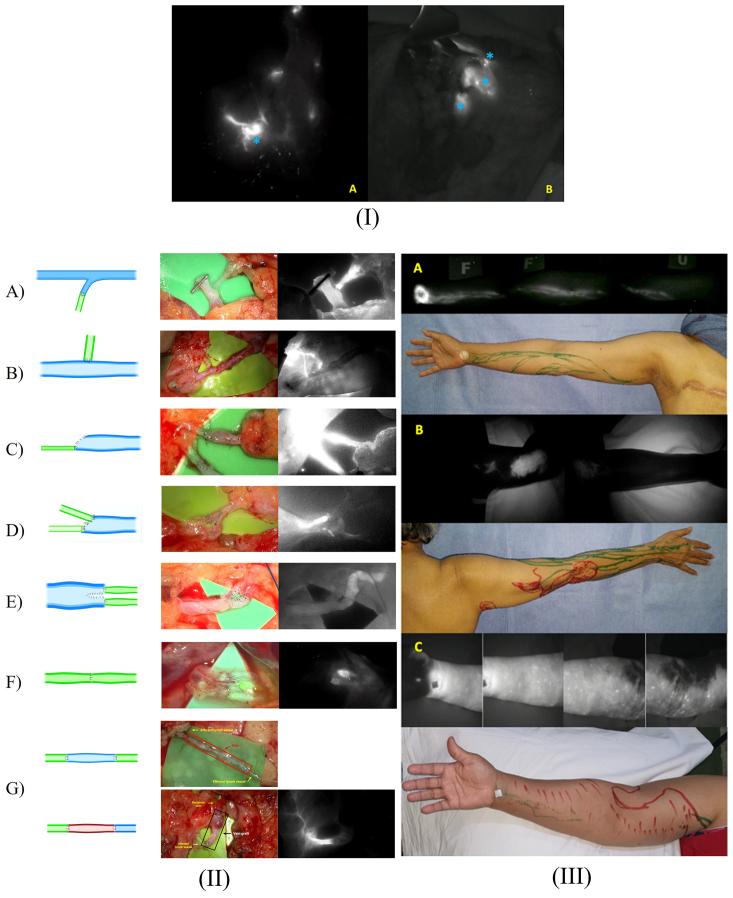
Methods: This study used a retrospective cohort design of patients with breast cancer between May 2020 and February 2023. LBS was performed by making an intima-to-intima coaptation between afferent lymph vessels and the recipient's veins (LVA) or efferent lymph vessels lymphaticolymphatic anastomosis.
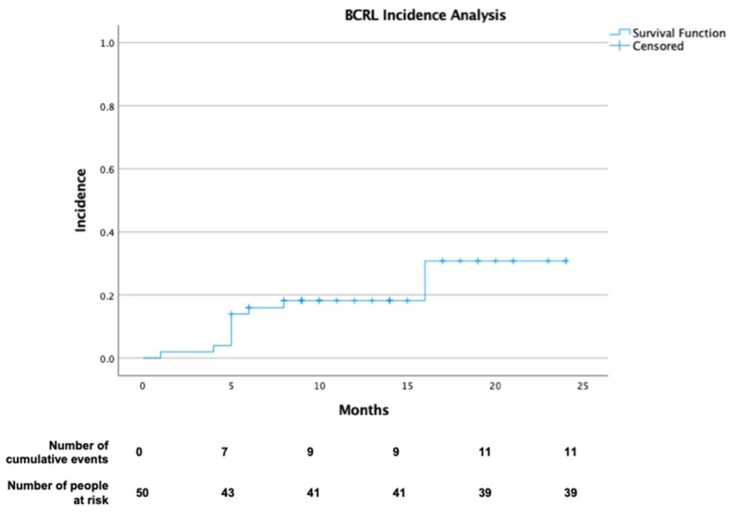
Results: A total of 82 patients underwent lymphatic bypass. The mean age of patients was 50 ± 12 years, and most had stage III breast cancer (n = 59 [72%]). LVA was the most common type of lymphatic bypass (94.6%). The median number of LVA was 1 (range, 1-4) and 1 (range, 1-3) for lymphaticolymphatic anastomosis. The median follow-up time was 12.5 months (range, 1-33 months). The 50 patients who had postoperative indocyanine green lymphography described arm dermal backflow stage 0 in 20 (40%), stage 1 in 19 (38%), stage 2 in 2 (4%), and stage 3 in 9 (18%) cases. The proportion of BCRL was 11 (22%), and subclinical lymphedema was 19 (38%) in this period. Most cases were in stable subclinical lymphedema (10, 58.8%). The 1-year and 2-year BCRL rates were 14% (95% confidence interval, 4%-23.9%) and 22% (95% confidence interval, 10.1%-33.9%), respectively.
Conclusions: Along with the emerging immediate lymphatic reconstruction, LBS is a feasible supermicrosurgery technique that may have a potential role in BCRL prevention. A randomized controlled study would confirm the effectiveness of the technique.
Keywords: Axillary lymph node dissection; Breast cancer; Immediate lymphatic reconstruction; Lymphedema; Supermicrosurgery.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures None.
Figures
References
-
- Boccardo F.M., Casabona F., Friedman D., et al. Surgical prevention of arm lymphedema after breast cancer treatment. Ann Surg Oncol. 2011;18:2500–2505. - PubMed
-
- Boccardo F., Casabona F., De Cian F., et al. Lymphatic microsurgical preventing healing approach (lympha) for primary surgical prevention of breast cancer-related lymphedema: over 4 years follow-up. Microsurgery. 2014;34:421–424. - PubMed
-
- Chun M.J., Saeg F., Meade A., et al. Immediate lymphatic reconstruction for prevention of secondary lymphedema: a meta-analysis. J Plast Reconstr Aesthet Surg. 2022;75:1130–1141. - PubMed
-
- Warren A.G., Brorson H., Borud L.J., Slavin S.A. Lymphedema: a comprehensive review. Ann Plast Surg. 2007;59:464–472. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
