

A tissue-silicone integrated simulator for right ventricular pulsatile circulation with severe functional tricuspid regurgitation
- PMID: 38429438
- PMCID: PMC10907752
- DOI: 10.1038/s41598-024-55058-w
A tissue-silicone integrated simulator for right ventricular pulsatile circulation with severe functional tricuspid regurgitation
Abstract
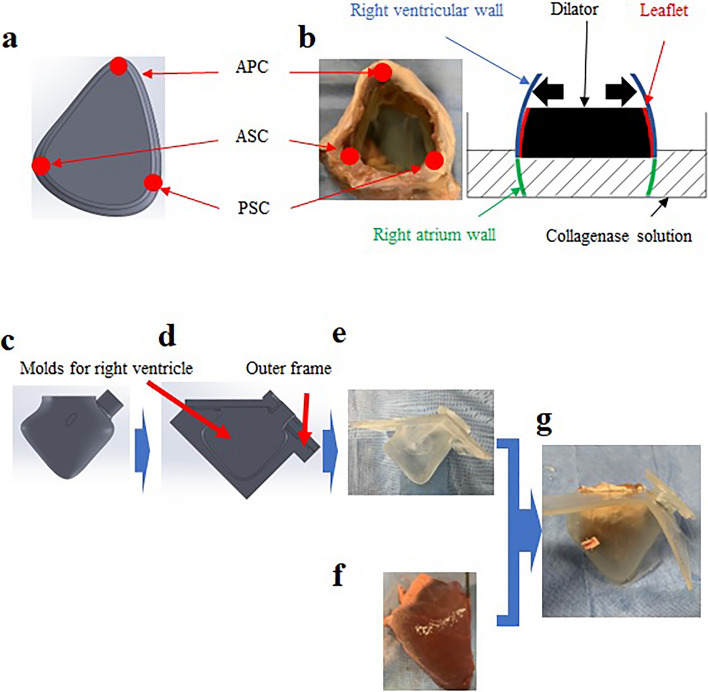
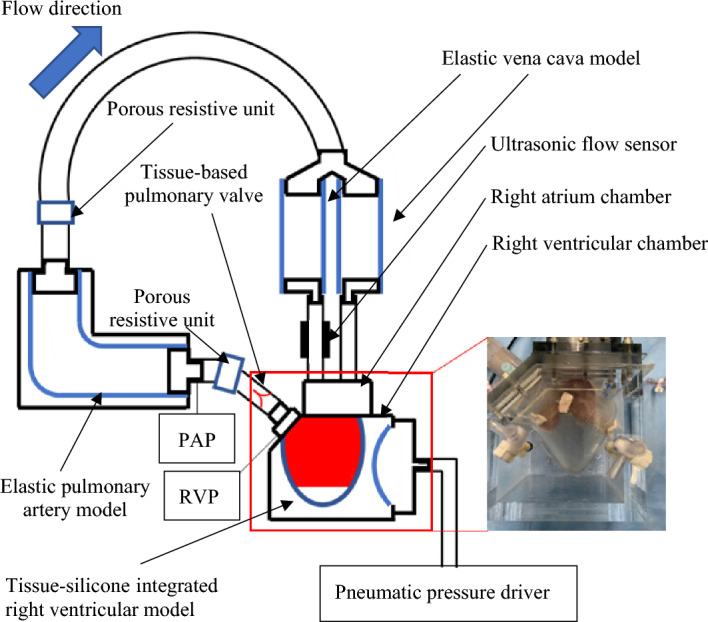
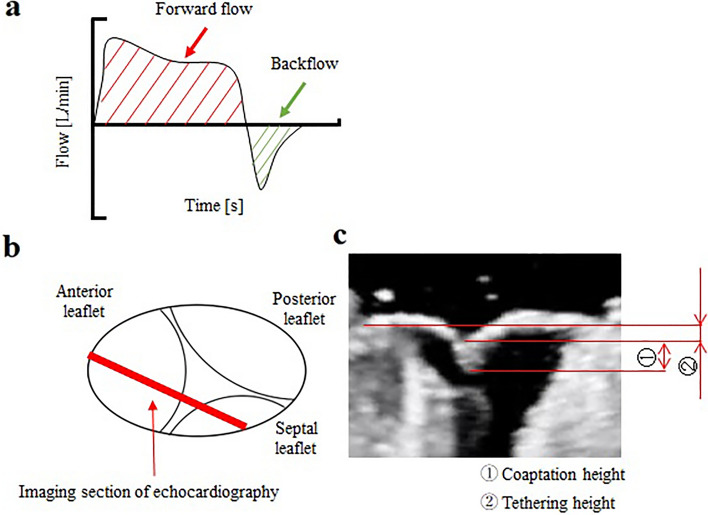
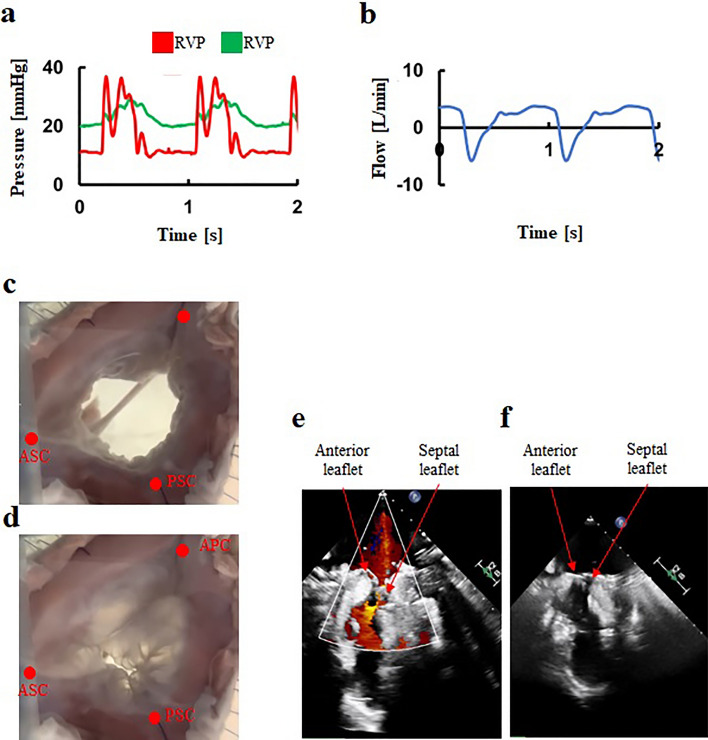
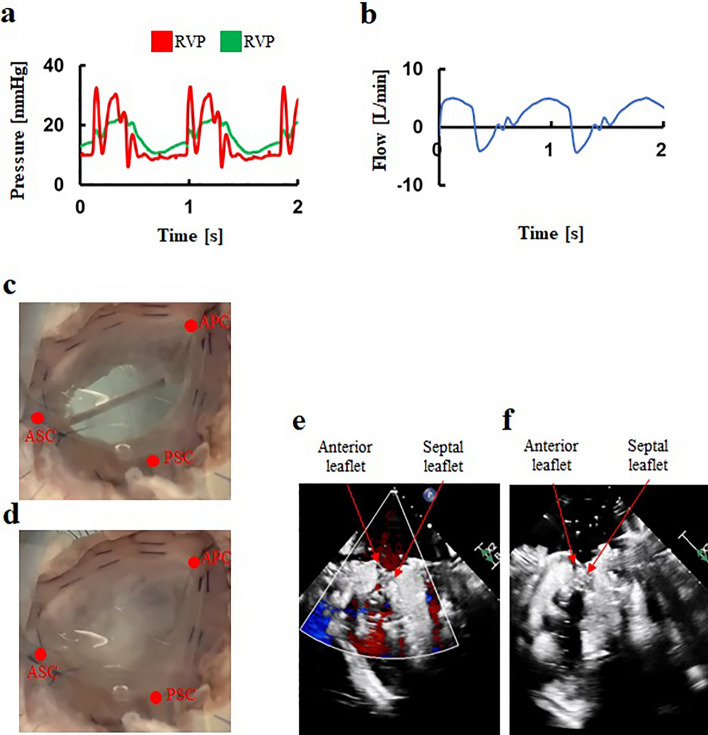
There is a great demand for development of a functional tricuspid regurgitation (FTR) model for accelerating development and preclinical study of tricuspid interventional repair devices. This study aimed to develop a severe FTR model by creating a tissue-silicone integrated right ventricular pulsatile circulatory simulator. The simulator incorporates the porcine tricuspid annulus, valve leaflets, chordae tendineae, papillary muscles, and right ventricular wall as one continuous piece of tissue, thereby preserving essential anatomical relationships of the tricuspid valve (TV) complex. We dilated the TV annulus with collagenolytic enzymes under applying stepwise dilation, and successfully achieved a severe FTR model with a regurgitant volume of 45 ± 9 mL/beat and a flow jet area of 15.8 ± 2.3 cm2 (n = 6). Compared to a normal model, the severe FTR model exhibited a larger annular circumference (133.1 ± 8.2 mm vs. 115.7 ± 5.5 mm; p = 0.009) and lower coaptation height (6.6 ± 1.0 mm vs. 17.7 ± 1.3 mm; p = 0.003). Following the De-Vega annular augmentation procedure to the severe FTR model, a significant reduction in regurgitant volume and flow jet area were observed. This severe FTR model may open new avenues for the development and evaluation of transcatheter TV devices.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
