

Delineating immune variation between adult and children COVID-19 cases and associations with disease severity
- PMID: 38429462
- PMCID: PMC10907598
- DOI: 10.1038/s41598-024-55148-9
Delineating immune variation between adult and children COVID-19 cases and associations with disease severity
Abstract
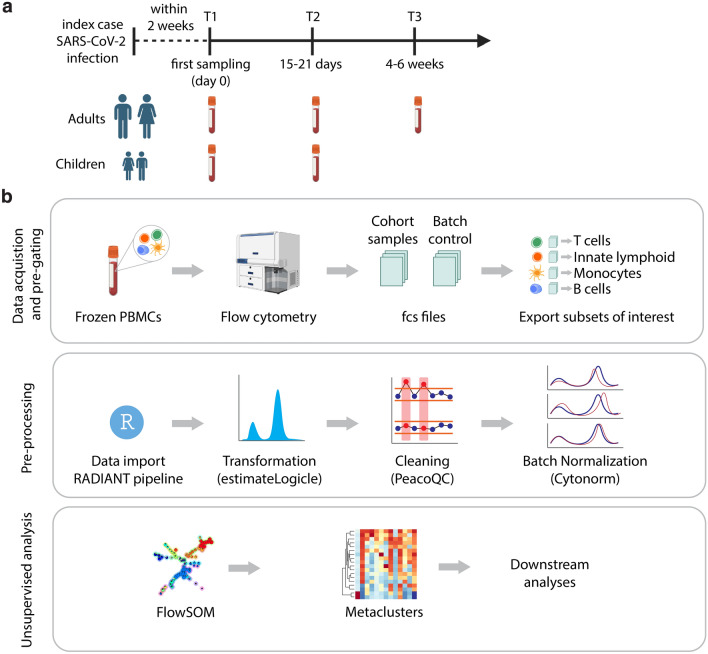
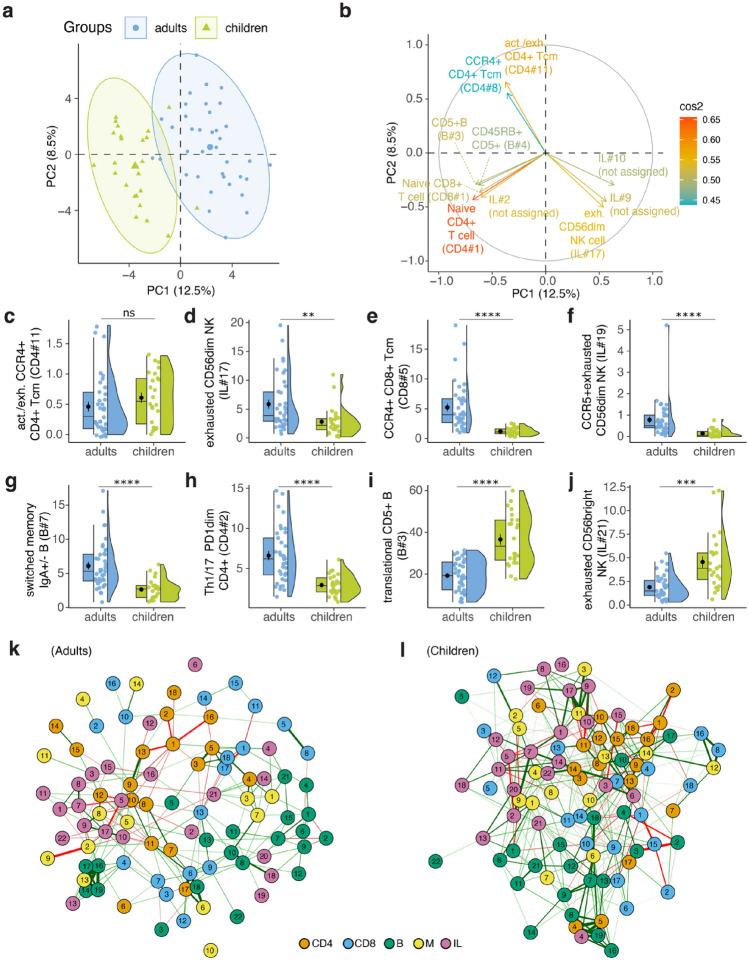
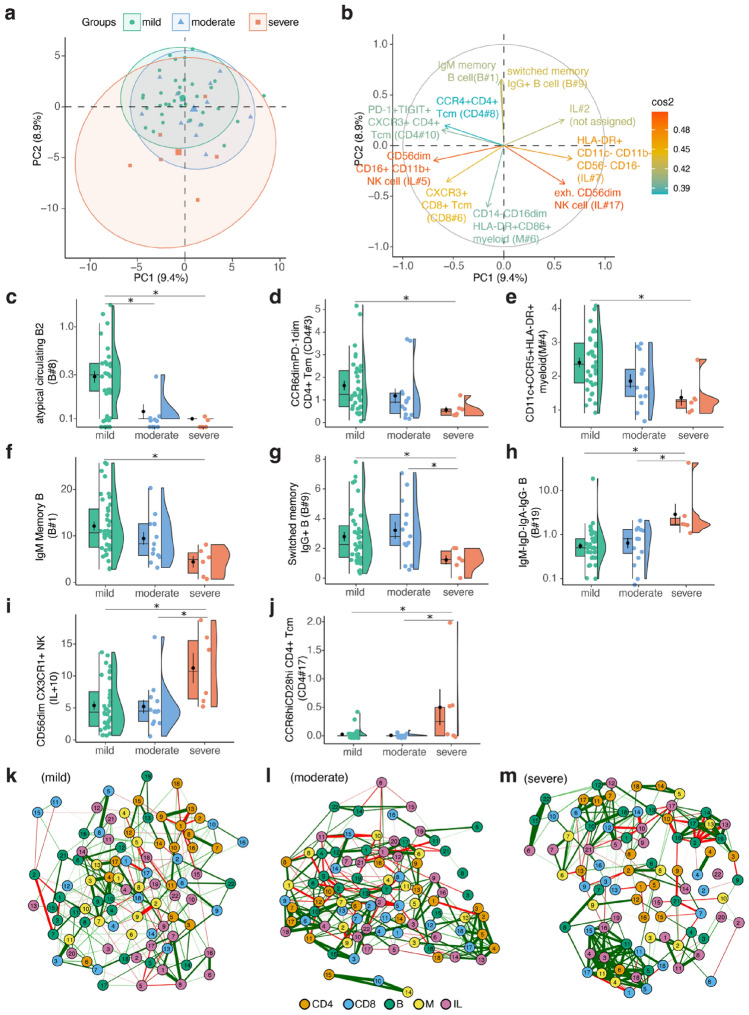
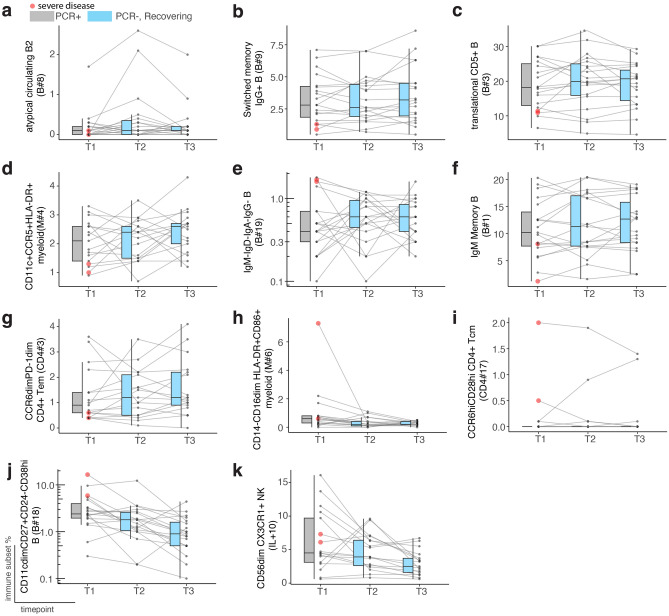
The SARS-CoV-2 pandemic has emphasized the need to explore how variations in the immune system relate to the severity of the disease. This study aimed to explore inter-individual variation in response to SARS-CoV-2 infection by comparing T cell, B cell, and innate cell immune subsets among primary infected children and adults (i.e., those who had never experienced SARS-CoV-2 infection nor received vaccination previously), with varying disease severity after infection. We also examined immune subset kinetics in convalescent individuals compared to those with persistent infection to identify possible markers of immune dysfunction. Distinct immune subset differences were observed between infected adults and children, as well as among adult cases with mild, moderate, and severe disease. IgM memory B cells were absent in moderate and severe cases whereas frequencies of B cells with a lack of surface immunoglobulin expression were significantly higher in severe cases. Interestingly, these immune subsets remained stable during recovery implying that these subsets could be associated with underlying baseline immune variation. Our results offer insights into the potential immune markers associated with severe COVID-19 and provide a foundation for future research in this area.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
