

Noninvasive Intracranial Pressure Monitoring: Are We There Yet?
- PMID: 38429611
- PMCID: PMC11377479
- DOI: 10.1007/s12028-024-01951-1
Noninvasive Intracranial Pressure Monitoring: Are We There Yet?
Abstract
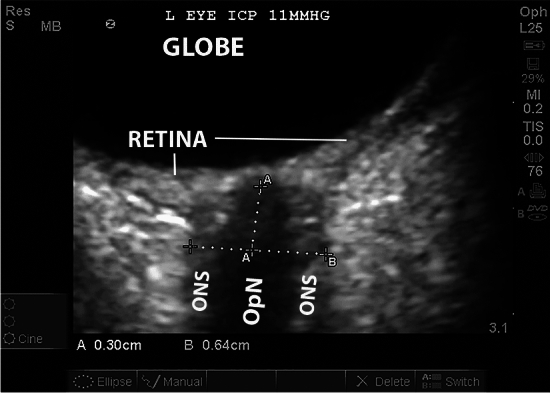
There is an urgent unmet need for a reliable noninvasive tool to detect elevations in intracranial pressure (ICP) above guideline-recommended thresholds for treatment. Gold standard invasive ICP monitoring is unavailable in many settings, including resource-limited environments, and in situations such as liver failure in which coagulopathy increases the risk of invasive monitoring. Although a large number of noninvasive techniques have been evaluated, this article reviews the potential clinical role, if any, of the techniques that have undergone the most extensive evaluation and are already in clinical use. Elevations in ICP transmitted through the subarachnoid space result in distension of the optic nerve sheath. The optic nerve sheath diameter (ONSD) can be measured with ultrasound, and an ONSD threshold can be used to detect elevated ICP. Although many studies suggest this technique accurately detects elevated ICP, there is concern for risk of bias and variations in ONSD thresholds across studies that preclude routine use of this technique in clinical practice. Multiple transcranial Doppler techniques have been used to assess ICP, but the best studied are the pulsatility index and the Czosnyka method to estimate cerebral perfusion pressure and ICP. Although there is inconsistency in the literature, recent prospective studies, including an international multicenter study, suggest the estimated ICP technique has a high negative predictive value (> 95%) but a poor positive predictive value (≤ 30%). Quantitative pupillometry is a sensitive and objective method to assess pupillary size and reactivity. Proprietary indices have been developed to quantify the pupillary light response. Limited data suggest these quantitative measurements may be useful for the early detection of ICP elevation. No current noninvasive technology can replace invasive ICP monitoring. Where ICP monitoring is unavailable, multimodal noninvasive assessment may be useful. Further innovation and research are required to develop a reliable, continuous technique of noninvasive ICP assessment.
Keywords: Acute brain injuries; Intracranial pressure; Optic nerve; Pupillary reflex; Transcranial Doppler ultrasonography.
© 2024. The Author(s).
Conflict of interest statement
There are no financial conflicts of interest to declare.
Figures



References
-
- Global Intracranial Pressure Monitoring Devices Market Size, Share, Growth Analysis, By Technique (Invasive, and Non-invasive), By Application (Traumatic Brain Injury, Intracerebral Hemorrhage)—Industry Forecast 2023–2030. 2023. https://www.skyquestt.com/report/intracranial-pressure-monitoring-device.... Accessed 13 Nov 2023.
MeSH terms
LinkOut - more resources
Full Text Sources
