

Radar-Guided Localization and Resection for Metastatic Nodal and Soft Tissue Melanoma: A Single-Institution Retrospective Study
- PMID: 38429650
- PMCID: PMC10908225
- DOI: 10.1177/10732748241237907
Radar-Guided Localization and Resection for Metastatic Nodal and Soft Tissue Melanoma: A Single-Institution Retrospective Study
Abstract
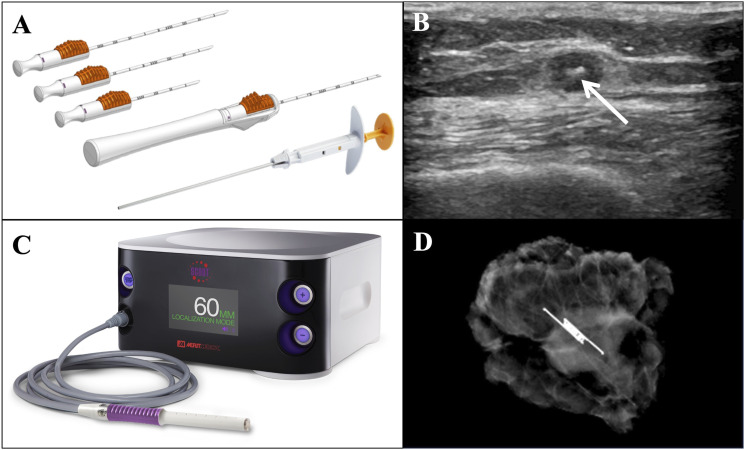
Background: Radar-guided localization (RGL) offers a wire-free, nonradioactive surgical guidance method consisting of a small percutaneously-placed radar reflector and handheld probe. This study investigates the feasibility, timing, and outcomes of RGL for melanoma metastasectomy.
Methods: We retrospectively identified patients at our cancer center who underwent RGL resection of metastatic melanoma between December 2020-June 2023. Data pertaining to patients' melanoma history, management, reflector placement and retrieval, and follow-up was extracted from patient charts and analyzed using descriptive statistics.
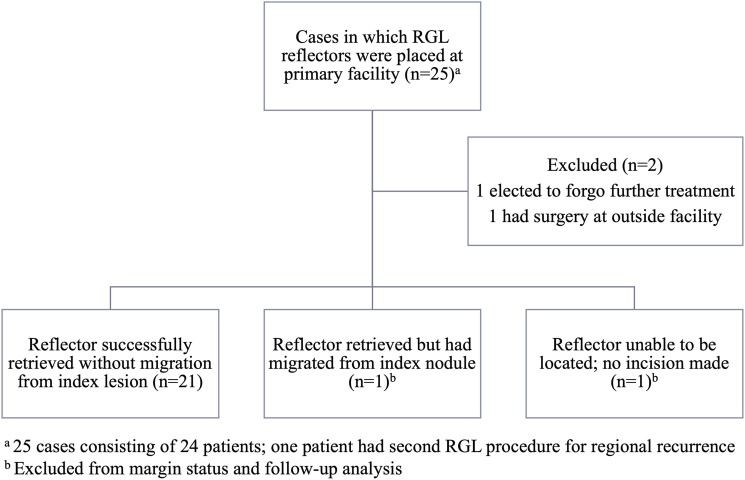
Results: Twenty-three RGL cases were performed in patients with stage III-IV locoregional or oligometastatic disease, 10 of whom had reflectors placed prior to neoadjuvant therapy. Procedures included soft tissue nodule removals (8), index lymph node removals (13), and therapeutic lymph node dissections (2). Reflectors were located and retrieved intraoperatively in 96% of cases from a range of 2 to 282 days after placement; the last reflector was not able to be located during surgery via probe or intraoperative ultrasound. One retrieved reflector had migrated from the index lesion, thus overall success rate of reflector and associated index lesion removal was 21 of 23 (91%). All RGL-localized and retrieved index lesions that contained viable tumor (10) had microscopically negative margins. There were no complications attributable to reflector insertion and no unexpected complications of RGL surgery.
Conclusion: In our practice, RGL is a safe and effective surgical localization method for soft tissue and nodal melanoma metastases. The inert nature of the reflector enables implantation prior to neoadjuvant therapy with utility in index lymph node removal.
Keywords: SAVI Scout; adjuvant therapy; cutaneous oncology; melanoma; metastatic melanoma lymph node dissection; neoadjuvant therapy; radar guided reflector; subcutaneous nodule; surgical guidance; tumor localization.
Plain language summary
There are a variety of tools available to localize melanoma that had spread to deep layers of the skin or lymph nodes that can guide surgeons to the cancer when the tumor cannot be felt. We evaluated a marker that reflects radar signals that has been studied in breast surgery but not in melanoma. The marker was placed in the tumor before surgery and was located during surgery using a handheld probe, guiding the surgeon to the correct location. An advantage of the radar-reflecting marker we studied is that since it is safe to stay in the body, it can be placed ahead of the use of cancer medications and can keep track of the tumor as it responds to treatment. In a review of 23 surgeries in which the radar-reflecting marker was used, there was one case where the marker migrated away from the tumor and one case where the marker was not able to be located. Monitoring or alternative definitive treatment was provided in each of these cases. Overall, we found the marker to be an effective tumor localization tool for surgeons and safe for patients. Other marker options available are unable or less suitable to be placed a long time in advance of surgery due to either technical or safety reasons, so the radar-reflecting marker is especially useful when it is placed in a tumor ahead of medical treatment leading up to planned surgical treatment.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Amod A Sarnaik is a co-inventor on a patent application with Provectus Biopharmaceuticals. Dr Sarnaik has received consulting fees from Iovance Biotherapeutics, Guidepoint, Defined Health, Huron Consulting Group, KeyQuest Health Inc, Istari, Rising Tide, and Gerson Lehrman Group. Dr Sarnaik has received speaker fees from the Society for Immunotherapy of Cancer, Physicians’ Educational Resource (PER) LLC, Medscape, and Medstar Health. Vernon K Sondak serves in a consulting or advisory role for Merck/Schering Plough, Novartis, Bristol Myers Squibb, Regeneron, Iovance Biotherapeutics, Alkermes, Ultimovacs, Genesis Drug Discovery and Development, and Sun Pharma. He has received research funding to the institution (Moffitt Cancer Center) from Neogene Therapeutics, Turnstone Bio, and Skyline Diagnostics, not related to this research. Jonathan S Zager has advisory board relationships with or has received fees from Merit Medical, Merck, Novartis, Philogen, Castle Biosciences, Pfizer, and Sun Pharma. He also received research funding from Amgen, Delcath Systems, Philogen, Provectus, and Novartis. He serves on the medical advisory board for Delcath Systems. John E Mullinax is an inventor on intellectual property that Moffitt Cancer Center has licensed to Iovance Biotherapeutics. He participates in sponsored research agreements with Iovance Biotherapeutics, Intellia Therapeutics, and SQZ Biotech that are not related to this research. He has received research support that is not related to this research from the following entities: NIH-NCI (K08CA252642), Ocala Royal Dames, and V Foundation. Dr Mullinax has received consulting fees from Merit Medical, Lyell Therapeutics, and Iovance Biotherapeutics. The remaining authors have no relevant conflicts of interest to disclose.
Figures
Similar articles
-
The Use of Radar-Guided Localization to Identify Metastatic Melanoma After Neoadjuvant Immunotherapy.Ann Surg Oncol. 2025 Jul;32(7):5300-5305. doi: 10.1245/s10434-025-17330-9. Epub 2025 Apr 25. Ann Surg Oncol. 2025. PMID: 40279056
-
Beyond Wires and Seeds: Reflector-guided Breast Lesion Localization and Excision.Radiology. 2017 Aug;284(2):365-371. doi: 10.1148/radiol.2017161661. Epub 2017 Apr 21. Radiology. 2017. PMID: 28430555
-
Ultrasound-guided radar reflector localization of axillary lymph nodes facilitates targeted axillary dissection.Clin Imaging. 2022 Oct;90:19-25. doi: 10.1016/j.clinimag.2022.07.007. Epub 2022 Jul 25. Clin Imaging. 2022. PMID: 35908456
-
Intraoperative Localization Using an Implanted Radar Reflector Facilitates Resection of Non-Palpable Trunk and Extremity Sarcoma.Ann Surg Oncol. 2021 Jun;28(6):3366-3374. doi: 10.1245/s10434-020-09229-4. Epub 2020 Oct 18. Ann Surg Oncol. 2021. PMID: 33073344 Review.
-
Savi-Scout Radar Localization: Transitioning From the Traditional Wire Localization to Wireless Technology for Surgical Guidance at Lumpectomies.Semin Ultrasound CT MR. 2023 Feb;44(1):12-17. doi: 10.1053/j.sult.2022.10.004. Epub 2022 Oct 22. Semin Ultrasound CT MR. 2023. PMID: 36792268 Review.
Cited by
-
The Use of Radar-Guided Localization to Identify Metastatic Melanoma After Neoadjuvant Immunotherapy.Ann Surg Oncol. 2025 Jul;32(7):5300-5305. doi: 10.1245/s10434-025-17330-9. Epub 2025 Apr 25. Ann Surg Oncol. 2025. PMID: 40279056
-
ASO Author Reflections: Successful Radar-Guided Localization for Targeted Melanoma Metastasectomy After Neoadjuvant Immunotherapy.Ann Surg Oncol. 2025 Jul;32(7):5319-5320. doi: 10.1245/s10434-025-17427-1. Epub 2025 May 9. Ann Surg Oncol. 2025. PMID: 40346411 No abstract available.
References
-
- NCCN . NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Melanoma: Cutaneous. NCCN; 2023.
-
- SCOUT® Surgical Guidance System Console Operation Manual; 2021. https://www.merit.com/wp-content/uploads/2021/06/SCOUT-Console-Operation...
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
