

Outcome measures in Angelman syndrome
- PMID: 38429713
- PMCID: PMC10905876
- DOI: 10.1186/s11689-024-09516-1
Outcome measures in Angelman syndrome
Abstract
Background: Angelman syndrome (AS) is a rare neurodevelopmental disorder characterized by severe intellectual disability, little to no expressive speech, visual and motor problems, emotional/behavioral challenges, and a tendency towards hyperphagia and weight gain. The characteristics of AS make it difficult to measure these children's functioning with standard clinical tests. Feasible outcome measures are needed to measure current functioning and change over time, in clinical practice and clinical trials.
Aim: Our first aim is to assess the feasibility of several functional tests. We target domains of neurocognitive functioning and physical growth using the following measurement methods: eye-tracking, functional Near-Infrared Spectroscopy (fNIRS), indirect calorimetry, bio-impedance analysis (BIA), and BOD POD (air-displacement plethysmography). Our second aim is to explore the results of the above measures, in order to better understand the AS phenotype.
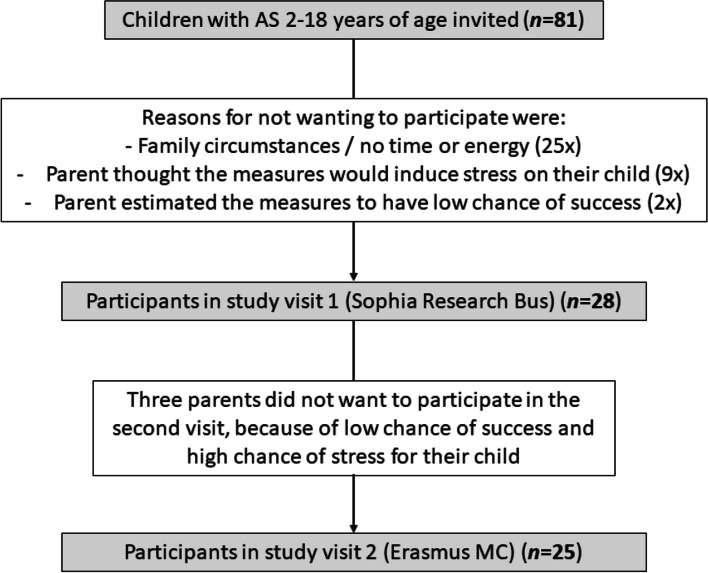
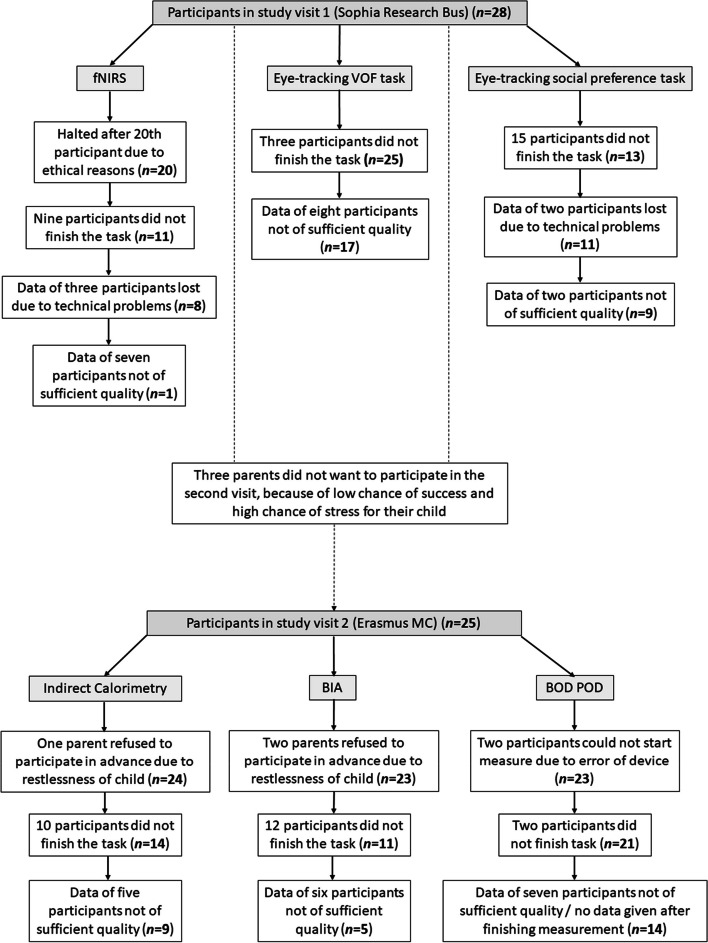
Methods: The study sample consisted of 28 children with AS aged 2-18 years. We defined an outcome measure as feasible when (1) at least 70% of participants successfully finished the measurement and (2) at least 60% of those participants had acceptable data quality. Adaptations to the test procedure and reasons for early termination were noted. Parents rated acceptability and importance and were invited to make recommendations to increase feasibility. The results of the measures were explored.
Results: Outcome measures obtained with eye-tracking and BOD POD met the definition of feasibility, while fNIRS, indirect calorimetry, and BIA did not. The most important reasons for early termination of measurements were showing signs of protest, inability to sit still and poor/no calibration (eye-tracking specific). Post-calibration was often applied to obtain valid eye-tracking results. Parents rated the BOD POD als most acceptable and fNIRS as least acceptable for their child. All outcome measures were rated to be important. Exploratory results indicated longer reaction times to high salient visual stimuli (eye-tracking) as well as high body fat percentage (BOD POD).
Conclusions: Eye-tracking and BOD POD are feasible measurement methods for children with AS. Eye-tracking was successfully used to assess visual orienting functions in the current study and (with some practical adaptations) can potentially be used to assess other outcomes as well. BOD POD was successfully used to examine body composition.
Trial registration: Registered d.d. 23-04-2020 under number 'NL8550' in the Dutch Trial Register: https://onderzoekmetmensen.nl/en/trial/23075.
Keywords: Angelman syndrome; BOD POD; Bio-impedance analysis; Eye-tracking; Functional near-Infrared Spectroscopy; Indirect calorimetry; Outcome measures.
© 2024. The Author(s).
Conflict of interest statement
MCdW is the Erasmus MC study site leader for the Roche Tangelo study, and the hospital received funding for this study. The hospital also received compensation for advice to Roche and Jazz Pharmaceuticals. The department of Child- and Adolescent Psychiatry/Psychology (Erasmus MC) is the Dutch distributer of the Achenbach System of Empirically Based Assessment (ASEBA) measurement instruments, which include the Child Behaviour Checklist (CBCL). The department receives financial compensation for selling the measurement instruments. All other authors have no conflict of interest to declare.
Figures
References
-
- Williams CA, Beaudet AL, Clayton-Smith J, Knoll JH, Kyllerman M, Laan LA, et al. Angelman syndrome 2005: updated consensus for diagnostic criteria. Am J Med Genet A. 2006;140A(5):413–418. - PubMed
-
- ClinicalTrials.gov. Identifier NCT04259281, a study of the safety and tolerability of GTX-102 in children with Angelman syndrome. Bethesda: National Library of Medicine (US); 2006; [about 6 screens]. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT04259281. Cited 2023 Jun 28.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
