

Accuracy of heart failure ascertainment using routinely collected healthcare data: a systematic review and meta-analysis
- PMID: 38429771
- PMCID: PMC10905869
- DOI: 10.1186/s13643-024-02477-5
Accuracy of heart failure ascertainment using routinely collected healthcare data: a systematic review and meta-analysis
Abstract
Background: Ascertainment of heart failure (HF) hospitalizations in cardiovascular trials is costly and complex, involving processes that could be streamlined by using routinely collected healthcare data (RCD). The utility of coded RCD for HF outcome ascertainment in randomized trials requires assessment. We systematically reviewed studies assessing RCD-based HF outcome ascertainment against "gold standard" (GS) methods to study the feasibility of using such methods in clinical trials.
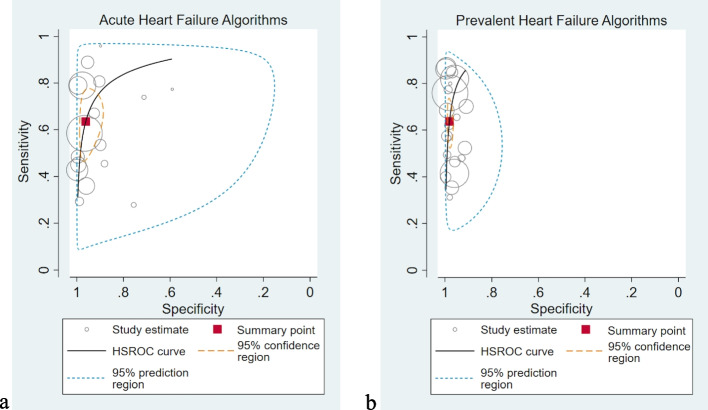
Methods: Studies assessing International Classification of Disease (ICD) coded RCD-based HF outcome ascertainment against GS methods and reporting at least one agreement statistic were identified by searching MEDLINE and Embase from inception to May 2021. Data on study characteristics, details of RCD and GS data sources and definitions, and test statistics were reviewed. Summary sensitivities and specificities for studies ascertaining acute and prevalent HF were estimated using a bivariate random effects meta-analysis. Heterogeneity was evaluated using I2 statistics and hierarchical summary receiver operating characteristic (HSROC) curves.
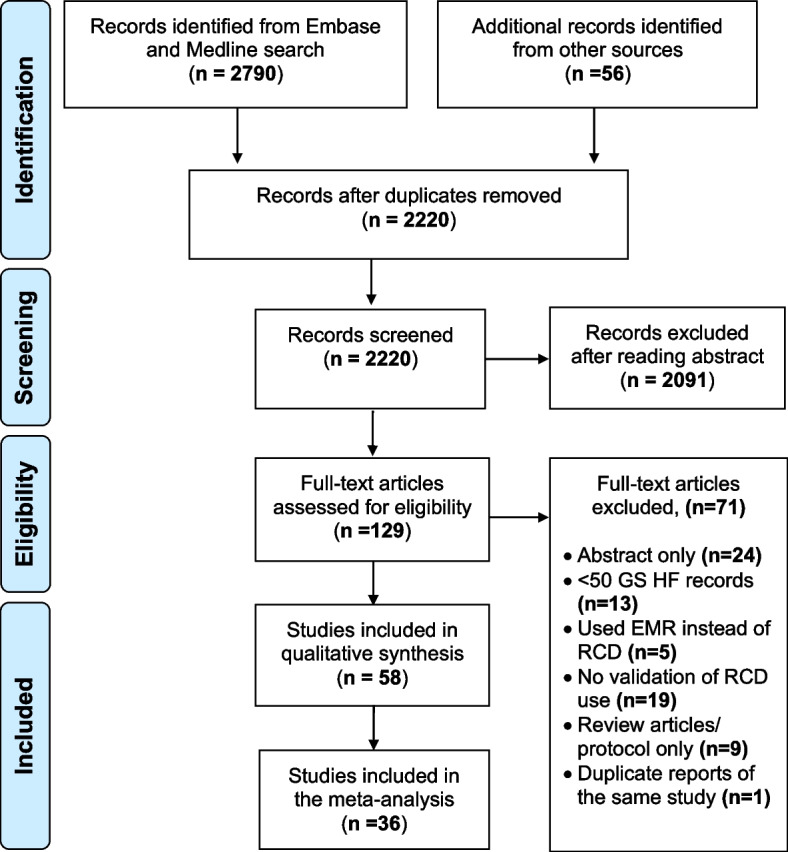
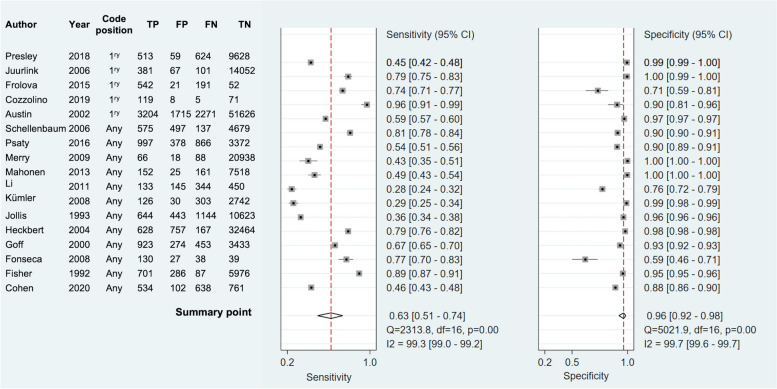
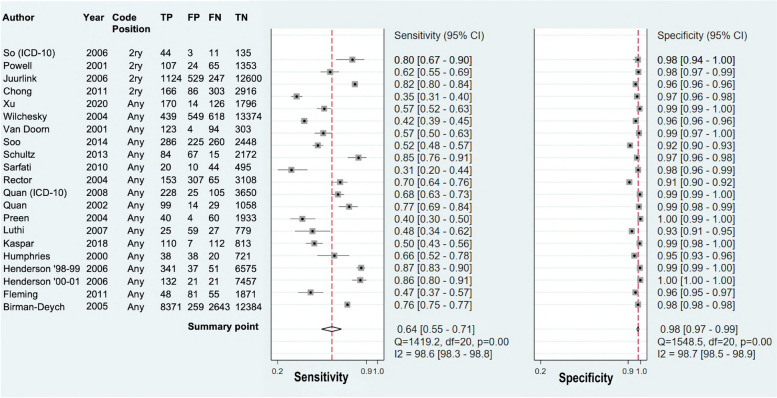
Results: A total of 58 studies of 48,643 GS-adjudicated HF events were included in this review. Strategies used to improve case identification included the use of broader coding definitions, combining multiple data sources, and using machine learning algorithms to search free text data, but these methods were not always successful and at times reduced specificity in individual studies. Meta-analysis of 17 acute HF studies showed that RCD algorithms have high specificity (96.2%, 95% confidence interval [CI] 91.5-98.3), but lacked sensitivity (63.5%, 95% CI 51.3-74.1) with similar results for 21 prevalent HF studies. There was considerable heterogeneity between studies.
Conclusions: RCD can correctly identify HF outcomes but may miss approximately one-third of events. Methods used to improve case identification should also focus on minimizing false positives.
Keywords: Meta-analysis; Methods comparison,; Outcome ascertainment,; Randomized trials,; Streamlined clinical trials,; Systematic review,.
© 2024. The Author(s).
Conflict of interest statement
S.P., M.M., A.O., R.H., M.G., WK, ME, and AEM work in the Clinical Trial Service Unit and Epidemiological Studies Unit of the Nuffield Department of Population Health at the University of Oxford. The Clinical Trial Service Unit and Epidemiological Studies Unit have a staff policy of not taking any personal payments directly or indirectly from industry (with reimbursement sought only for the costs of travel and accommodation to attend scientific meetings). It has received research grants from Abbott, AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline, The Medicines Company, Merck, Mylan, Novartis, Novo Nordisk, Pfizer, Roche, Schering, and Solvay, which are governed by University of Oxford contracts that protect their independence.
Figures
References
-
- McMurray JJ, Pfeffer MA. Heart failure. Lancet. 2005;365(9474):1877–1889. - PubMed
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. - PMC - PubMed
-
- Bragazzi NL, Zhong W, Shu J, Abu Much A, Lotan D, Grupper A, et al. Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur J Prev Cardiol. 2021;28(15):1682–1690. - PubMed
-
- Sertkaya A, Wong HH, Jessup A, Beleche T. Key cost drivers of pharmaceutical clinical trials in the United States. Clin Trials. 2016;13(2):117–126. - PubMed
-
- Speich B, von Niederhäusern B, Schur N, Hemkens LG, Fürst T, Bhatnagar N, et al. Systematic review on costs and resource use of randomized clinical trials shows a lack of transparent and comprehensive data. J Clin Epidemiol. 2018;96:1–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
