

Impact of late gadolinium enhancement image acquisition resolution on neural network based automatic scar segmentation
- PMID: 38431078
- PMCID: PMC10981112
- DOI: 10.1016/j.jocmr.2024.101031
Impact of late gadolinium enhancement image acquisition resolution on neural network based automatic scar segmentation
Abstract
Background: Automatic myocardial scar segmentation from late gadolinium enhancement (LGE) images using neural networks promises an alternative to time-consuming and observer-dependent semi-automatic approaches. However, alterations in data acquisition, reconstruction as well as post-processing may compromise network performance. The objective of the present work was to systematically assess network performance degradation due to a mismatch of point-spread function between training and testing data.
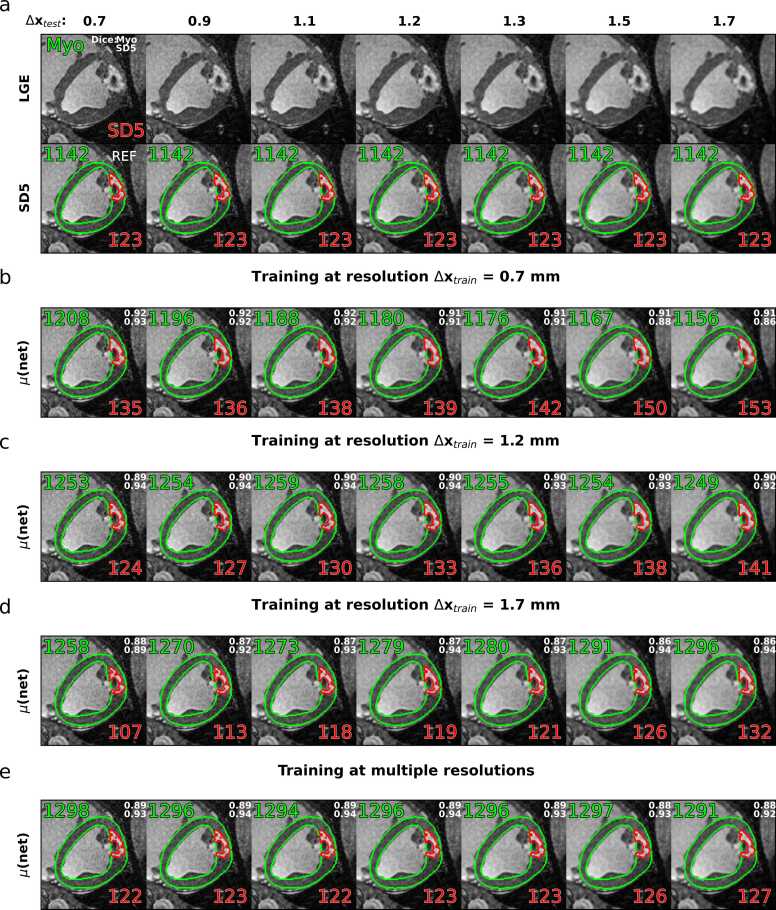
Methods: Thirty-six high-resolution (0.7×0.7×2.0 mm3) LGE k-space datasets were acquired post-mortem in porcine models of myocardial infarction. The in-plane point-spread function and hence in-plane resolution Δx was retrospectively degraded using k-space lowpass filtering, while field-of-view and matrix size were kept constant. Manual segmentation of the left ventricle (LV) and healthy remote myocardium was performed to quantify location and area (% of myocardium) of scar by thresholding (≥ SD5 above remote). Three standard U-Nets were trained on training resolutions Δxtrain = 0.7, 1.2 and 1.7 mm to predict endo- and epicardial borders of LV myocardium and scar. The scar prediction of the three networks for varying test resolutions (Δxtest = 0.7 to 1.7 mm) was compared against the reference SD5 thresholding at 0.7 mm. Finally, a fourth network trained on a combination of resolutions (Δxtrain = 0.7 to 1.7 mm) was tested.
Results: The prediction of relative scar areas showed the highest precision when the resolution of the test data was identical to or close to the resolution used during training. The median fractional scar errors and precisions (IQR) from networks trained and tested on the same resolution were 0.0 percentage points (p.p.) (1.24 - 1.45), and - 0.5 - 0.0 p.p. (2.00 - 3.25) for networks trained and tested on the most differing resolutions, respectively. Deploying the network trained on multiple resolutions resulted in reduced resolution dependency with median scar errors and IQRs of 0.0 p.p. (1.24 - 1.69) for all investigated test resolutions.
Conclusion: A mismatch of the imaging point-spread function between training and test data can lead to degradation of scar segmentation when using current U-Net architectures as demonstrated on LGE porcine myocardial infarction data. Training networks on multi-resolution data can alleviate the resolution dependency.
Keywords: Automatic segmentation; Cardiovascular magnetic resonance; Deep learning; LGE imaging; Neural networks; Scar quantification.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Not applicable reports financial support was provided by Innosuisse Swiss Innovation Agency. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures





References
-
- Puntmann V.O., Valbuena S., Hinojar R., et al. Society for Cardiovascular Magnetic Resonance (SCMR) expert consensus for CMR imaging endpoints in clinical research: part I - analytical validation and clinical qualification. J Cardiovasc Magn Reson. 2018;20:1–23. doi: 10.1186/S12968-018-0484-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
