doi: 10.3988/jcn.2023.0332.
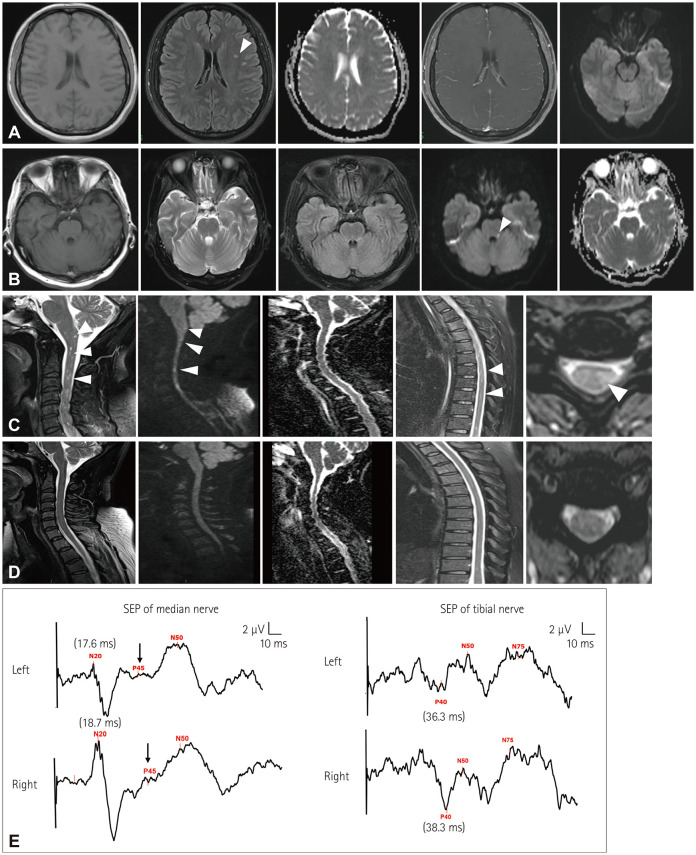
Atypical Meningoencephalomyelitis Following Varicella Zoster Virus Infection
Affiliations
- PMID: 38433487
- PMCID: PMC10921040
- DOI: 10.3988/jcn.2023.0332
Item in Clipboard
Atypical Meningoencephalomyelitis Following Varicella Zoster Virus Infection
J Clin Neurol.
2024 Mar.
No abstract available
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- McKelvie PA, Collins S, Thyagarajan D, Trost N, Sheorey H, Byrne E. Meningoencephalomyelitis with vasculitis due to varicella zoster virus: a case report and review of the literature. Pathology. 2002;34:88–93. - PubMed
-
- Tenembaum S, Chitnis T, Ness J, Hahn JS International Pediatric MS Study Group. Acute disseminated encephalomyelitis. Neurology. 2007;68(16 Suppl 2):S23–S36. - PubMed
-
- Trebst C, Raab P, Voss EV, Rommer P, Abu-Mugheisib M, Zettl UK, et al. Longitudinal extensive transverse myelitis--it’s not all neuromyelitis optica. Nat Rev Neurol. 2011;7:688–698. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources