

Carboxyhemoglobin half-life toxicokinetic profiles during and after normobaric oxygen therapy: On a swine model
- PMID: 38433766
- PMCID: PMC10907397
- DOI: 10.1016/j.toxrep.2024.02.005
Carboxyhemoglobin half-life toxicokinetic profiles during and after normobaric oxygen therapy: On a swine model
Abstract
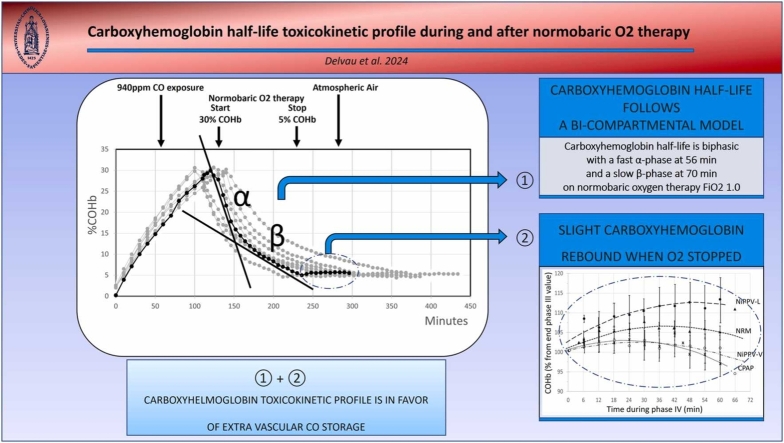
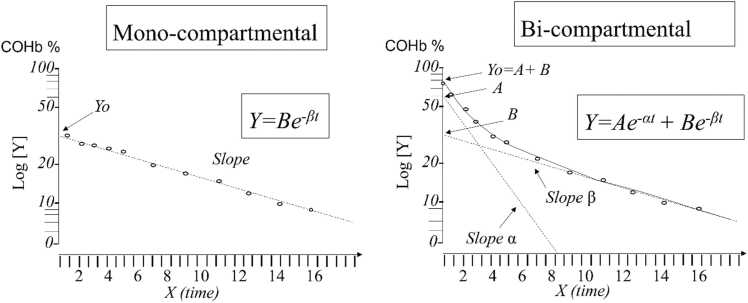
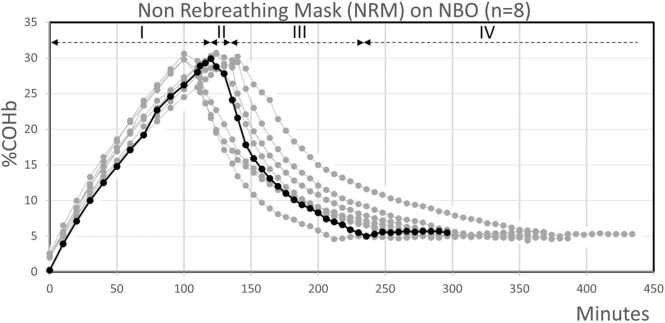
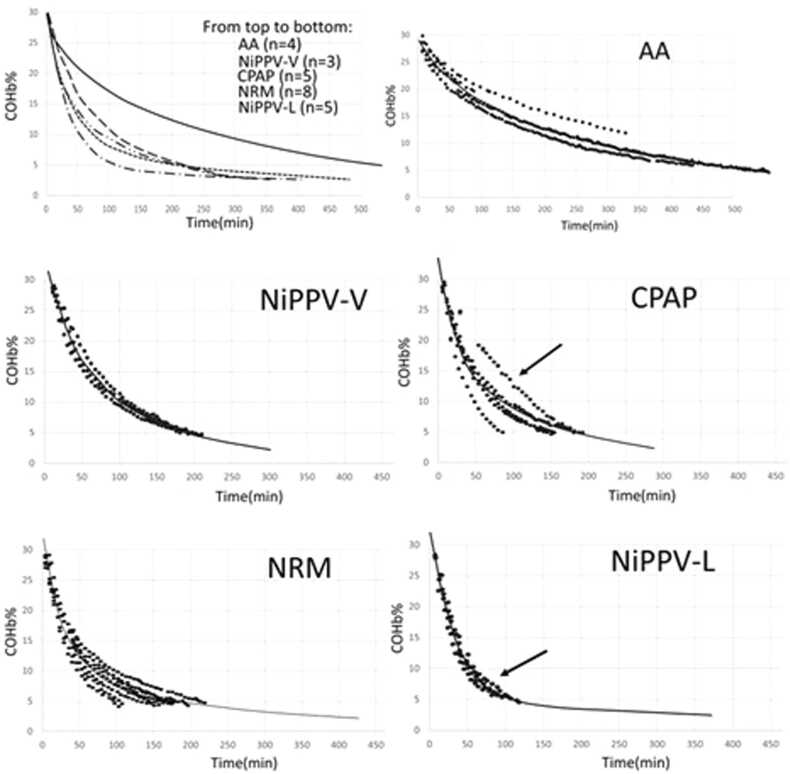
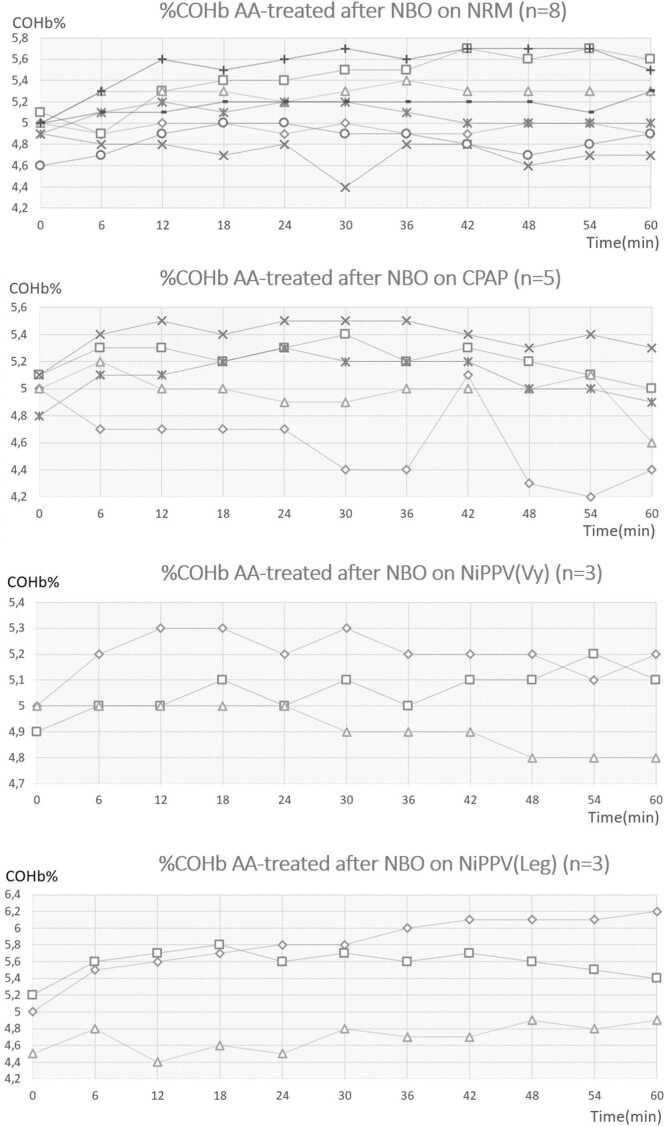
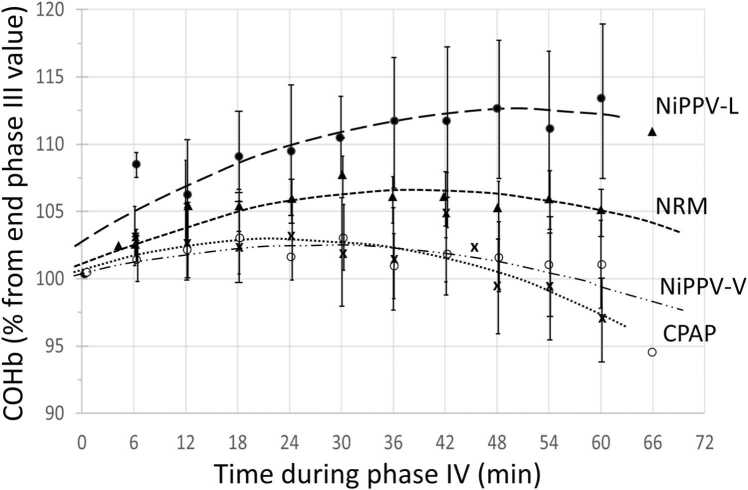
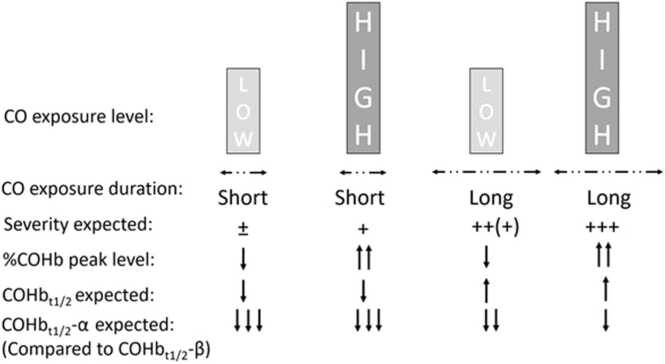
Investigations on acute carbon monoxide (CO) poisoning struggle to highlight a relevant discriminant criterion related to CO poisoning severity for predicting complications, such as delayed neurological syndromes. In this context, it remains difficult to demonstrate the superiority of one method of oxygen (O2) administration over others or to identify the optimal duration of normobaric 100% oxygen (NBO) treatment. Myoglobin, as hemoglobin, are a potential binding site for CO, which could be a source of extravascular CO storage that impacts the severity of CO poisoning. It is not possible in routine clinical practice to estimate this potential extravascular CO storage. Indirect means of doing so that are available in the first few hours of poisoning could include, for example, the carboxyhemoglobin half-life (COHbt1/2), which seems to be influenced itself by the level and duration of CO exposure affecting this store of CO within the body. However, before the elimination of CO can be assessed, the COHbt1/2 toxicokinetic model must be confirmed: research still debates whether this model mono- or bi-compartmental. The second indirect mean could be the assessment of a potential COHb rebound after COHb has returned to 5% and NBO treatment has stopped. Moreover, a COHb rebound could be considered to justify the duration of NBO treatment. On an experimental swine model exposed to moderate CO poisoning (940 ppm for ±118 min until COHb reached 30%), we first confirm that the COHb half-life follows a bi-compartmental model. Secondly, we observe for the first time a slight COHb rebound when COHb returns to 5% and oxygen therapy is stopped. On the basis of these two toxicokinetic characteristics in favor of extravascular CO storage, we recommend that COHbt1/2 is considered using the bi-compartmental model in future clinical studies that compare treatment effectiveness as a potential severity criterion to homogenize cohorts of the same severity. Moreover, from a general toxicokinetic point of view, we confirm that a treatment lasting less than 6 hours appears to be insufficient for treating moderate CO poisoning.
Keywords: Carbon monoxide; Carbon monoxide poisoning management; Carboxyhemoglobin (COHb); Carboxyhemoglobin half-life (COHbt1/2); Swine; Toxicokinetics.
© 2024 Published by Elsevier B.V.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Delvau Nicolas reports financial support was provided by Vygon. Delvau Nicolas reports financial support was provided by Saint-Luc Foundation.
Figures
Similar articles
-
Effect of Pressure Support Ventilation on Carboxyhemoglobin Toxicokinetic after Acute Carbon Monoxide Intoxication: a Swine Model.J Med Toxicol. 2018 Jun;14(2):128-133. doi: 10.1007/s13181-018-0654-8. Epub 2018 Feb 21. J Med Toxicol. 2018. PMID: 29468519 Free PMC article.
-
On half-clearance time of carbon monoxide hemoglobin in blood during hyperbaric oxygen therapy (OHP).Bull Tokyo Med Dent Univ. 1975 Mar;22(1):63-77. Bull Tokyo Med Dent Univ. 1975. PMID: 1055025
-
Extracorporeal membrane oxygenators with light-diffusing fibers for treatment of carbon monoxide poisoning: Experiments, mathematical modeling, and performance assessment with unit cells.Lasers Surg Med. 2023 Aug;55(6):590-600. doi: 10.1002/lsm.23673. Epub 2023 May 30. Lasers Surg Med. 2023. PMID: 37253390
-
A review of the experimental evidence on the toxicokinetics of carbon monoxide: the potential role of pathophysiology among susceptible groups.Environ Health. 2018 Feb 5;17(1):13. doi: 10.1186/s12940-018-0357-2. Environ Health. 2018. PMID: 29402286 Free PMC article. Review.
-
Carboxyhemoglobin half-life in carbon monoxide-poisoned patients treated with 100% oxygen at atmospheric pressure.Chest. 2000 Mar;117(3):801-8. doi: 10.1378/chest.117.3.801. Chest. 2000. PMID: 10713010 Review.
Cited by
-
Carbon Monoxide: A Pleiotropic Redox Regulator of Life and Death.Antioxidants (Basel). 2024 Sep 16;13(9):1121. doi: 10.3390/antiox13091121. Antioxidants (Basel). 2024. PMID: 39334780 Free PMC article. Review.
-
Carbon Monoxide and Prokaryotic Energy Metabolism.Int J Mol Sci. 2025 Mar 20;26(6):2809. doi: 10.3390/ijms26062809. Int J Mol Sci. 2025. PMID: 40141451 Free PMC article. Review.
References
-
- Mattiuzzi C., Lippi G. Worldwide epidemiology of carbon monoxide poisoning. Hum. Exp. Toxicol. 2020;39(4):387–392. - PubMed
-
- Juurlink D. Hyperbaric oxygen should not be used routinely for carbon monoxide poisoning: CON. Authorea Preprints. 2022. - PubMed
-
- Weaver L.K., Hopkins R.O., Chan K.J., Churchill S., Elliott C.G., Clemmer T.P., et al. Hyperbaric oxygen for acute carbon monoxide poisoning. N. Engl. J. Med. 2002;347(14):1057–1067. - PubMed
-
- Wolf S.J., Maloney G.E., Shih R.D., Shy B.D., Brown M.D. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with acute carbon monoxide poisoning. Ann. Emerg. Med. 2017;69(1):98–107. e6. - PubMed
LinkOut - more resources
Full Text Sources
