

Skeletal Muscle Evaluation in Patients With Acromegaly
- PMID: 38434516
- PMCID: PMC10907006
- DOI: 10.1210/jendso/bvae032
Skeletal Muscle Evaluation in Patients With Acromegaly
Abstract
Context: Patients with acromegaly are characterized by chronic exposure to high growth hormone (GH) and insulin-like growth factor-1 levels, known for their anabolic effect on skeletal muscle. Therefore, an increased skeletal muscle mass could be hypothesized in these individuals. Herein, we have performed a systematic revision of published evidence regarding skeletal muscle mass, quality, and performance in patients with acromegaly.
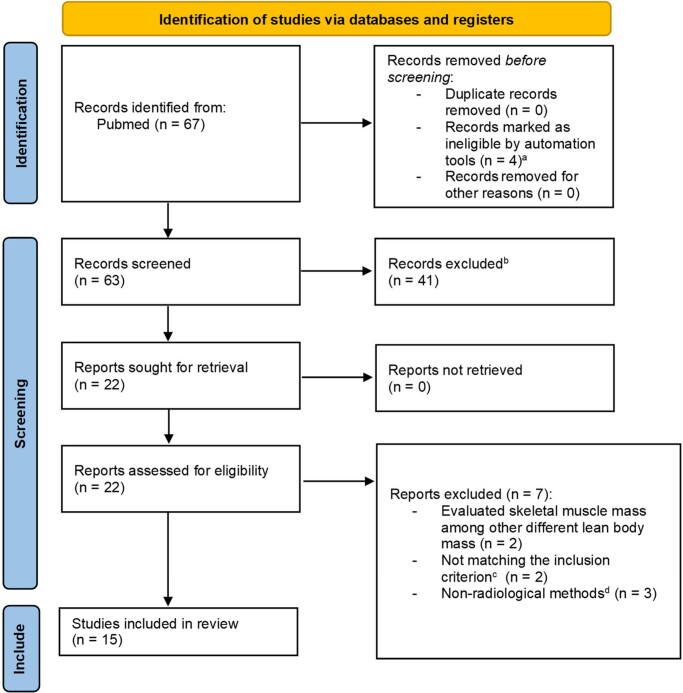
Evidence acquisition: A systematic review of the literature in the PubMed database up to September 1, 2023, was conducted with the following query: acromegaly AND ("muscle mass" OR "skeletal muscle"). We excluded studies that did not compare different disease states or used nonradiological methods for the skeletal muscle analyses, except for bioelectrical impedance analysis.
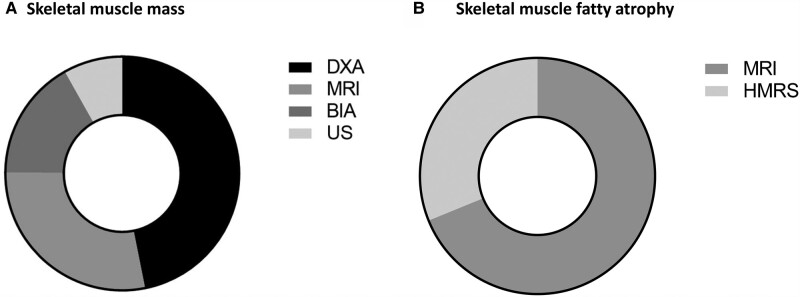
Evidence synthesis: Fifteen studies met the inclusion criteria. A total of 360 patients were evaluated for skeletal muscle mass, 122 for muscle fatty atrophy, and 192 for muscle performance. No clear evidence of increased skeletal muscle mass in patients with active disease compared to control or healthy individuals emerged. As for skeletal muscle quality, we observed a trend toward higher fatty infiltration among patients with acromegaly compared to healthy participants. Likewise, patients with active disease showed consistently worse physical performance compared to control or healthy individuals.
Conclusion: Skeletal muscle in acromegaly has lower quality and performance compared to that of healthy individuals. The small number of published studies and multiple confounding factors (eg, use of different radiological techniques) contributed to mixed results, especially regarding skeletal muscle mass. Well-designed prospective studies are needed to investigate skeletal muscle mass in patients with acromegaly.
Keywords: acromegaly; function; mass; myopathy; quality; skeletal muscle.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society.
Figures

Similar articles
-
Reversible insulin resistance in muscle and fat unrelated to the metabolic syndrome in patients with acromegaly.EBioMedicine. 2022 Jan;75:103763. doi: 10.1016/j.ebiom.2021.103763. Epub 2021 Dec 17. EBioMedicine. 2022. PMID: 34929488 Free PMC article.
-
Skeletal muscle sodium and potassium changes after successful surgery in acromegaly: relation to body composition, blood glucose, plasma insulin and blood pressure.Acta Endocrinol (Copenh). 1993 May;128(5):418-22. doi: 10.1530/acta.0.1280418. Acta Endocrinol (Copenh). 1993. PMID: 8317188
-
Whole-Body and Forearm Muscle Protein Metabolism in Patients With Acromegaly Before and After Treatment.J Clin Endocrinol Metab. 2023 Aug 18;108(9):e671-e678. doi: 10.1210/clinem/dgad190. J Clin Endocrinol Metab. 2023. PMID: 37036819
-
Acromegaly as an endocrine form of myopathy: case report and review of literature.Endocr Pract. 2005 Jan-Feb;11(1):18-22. doi: 10.4158/EP.11.1.18. Endocr Pract. 2005. PMID: 16033731 Review.
-
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND AMERICAN COLLEGE OF ENDOCRINOLOGY DISEASE STATE CLINICAL REVIEW: MANAGEMENT OF ACROMEGALY PATIENTS: WHAT IS THE ROLE OF PRE-OPERATIVE MEDICAL THERAPY?Endocr Pract. 2015 Jun;21(6):668-73. doi: 10.4158/EP14575.DSCR. Endocr Pract. 2015. PMID: 26135961 Review.
Cited by
-
Body Composition, Sarcopenia, and Serum Myokines in Acromegaly: A Narrative Review.J Bone Metab. 2024 Aug;31(3):182-195. doi: 10.11005/jbm.2024.31.3.182. Epub 2024 Aug 31. J Bone Metab. 2024. PMID: 39307519 Free PMC article.
-
Temporal and masseter muscle evaluation by MRI provides information on muscle mass and quality in acromegaly patients.Pituitary. 2024 Oct;27(5):507-517. doi: 10.1007/s11102-024-01422-y. Epub 2024 Jul 5. Pituitary. 2024. PMID: 38967765 Free PMC article.
-
A Case of Acromegaly With Progressed Diabetic Retinopathy and Sarcopenia Diagnosed Following the Onset of Severe Hypoglycemia.Cureus. 2024 Apr 17;16(4):e58461. doi: 10.7759/cureus.58461. eCollection 2024 Apr. Cureus. 2024. PMID: 38765413 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous