

Direct three-dimensional segmentation of prostate glands with nnU-Net
- PMID: 38434772
- PMCID: PMC10905031
- DOI: 10.1117/1.JBO.29.3.036001
Direct three-dimensional segmentation of prostate glands with nnU-Net
Abstract
Significance: In recent years, we and others have developed non-destructive methods to obtain three-dimensional (3D) pathology datasets of clinical biopsies and surgical specimens. For prostate cancer risk stratification (prognostication), standard-of-care Gleason grading is based on examining the morphology of prostate glands in thin 2D sections. This motivates us to perform 3D segmentation of prostate glands in our 3D pathology datasets for the purposes of computational analysis of 3D glandular features that could offer improved prognostic performance.
Aim: To facilitate prostate cancer risk assessment, we developed a computationally efficient and accurate deep learning model for 3D gland segmentation based on open-top light-sheet microscopy datasets of human prostate biopsies stained with a fluorescent analog of hematoxylin and eosin (H&E).
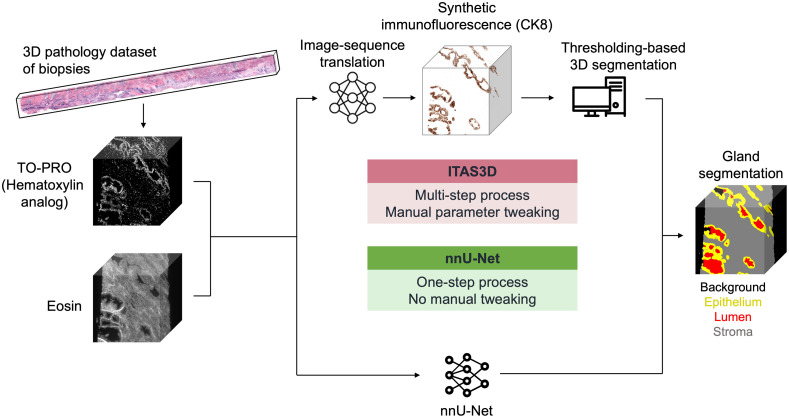
Approach: For 3D gland segmentation based on our H&E-analog 3D pathology datasets, we previously developed a hybrid deep learning and computer vision-based pipeline, called image translation-assisted segmentation in 3D (ITAS3D), which required a complex two-stage procedure and tedious manual optimization of parameters. To simplify this procedure, we use the 3D gland-segmentation masks previously generated by ITAS3D as training datasets for a direct end-to-end deep learning-based segmentation model, nnU-Net. The inputs to this model are 3D pathology datasets of prostate biopsies rapidly stained with an inexpensive fluorescent analog of H&E and the outputs are 3D semantic segmentation masks of the gland epithelium, gland lumen, and surrounding stromal compartments within the tissue.
Results: nnU-Net demonstrates remarkable accuracy in 3D gland segmentations even with limited training data. Moreover, compared with the previous ITAS3D pipeline, nnU-Net operation is simpler and faster, and it can maintain good accuracy even with lower-resolution inputs.
Conclusions: Our trained DL-based 3D segmentation model will facilitate future studies to demonstrate the value of computational 3D pathology for guiding critical treatment decisions for patients with prostate cancer.
Keywords: biomedical image processing; computational three-dimensional pathology; deep learning; gland segmentation; prostate cancer.
© 2024 The Authors.
Figures




References
-
- Shah R. B., et al. , “Improvement of diagnostic agreement among pathologists in resolving an “atypical glands suspicious for cancer” diagnosis in prostate biopsies using a novel “Disease-Focused Diagnostic Review” quality improvement process,” Hum. Pathol. 56, 155–162 (2016).HPCQA410.1016/j.humpath.2016.06.009 - DOI - PubMed
-
- Kane C. J., et al. , “Variability in outcomes for patients with intermediate-risk prostate cancer (Gleason Score 7, International Society of Urological Pathology Gleason Group 2–3) and implications for risk stratification: a systematic review,” Eur. Urol. Focus 3, 487–497 (2017).10.1016/j.euf.2016.10.010 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
