

A complex case of necrotizing pneumonia and parapneumonic effusion in a healthy 20-month-old child: Successful management with video-assisted thoracoscopic surgery and chest tube placement
- PMID: 38434785
- PMCID: PMC10907134
- DOI: 10.1016/j.radcr.2024.02.005
A complex case of necrotizing pneumonia and parapneumonic effusion in a healthy 20-month-old child: Successful management with video-assisted thoracoscopic surgery and chest tube placement
Abstract
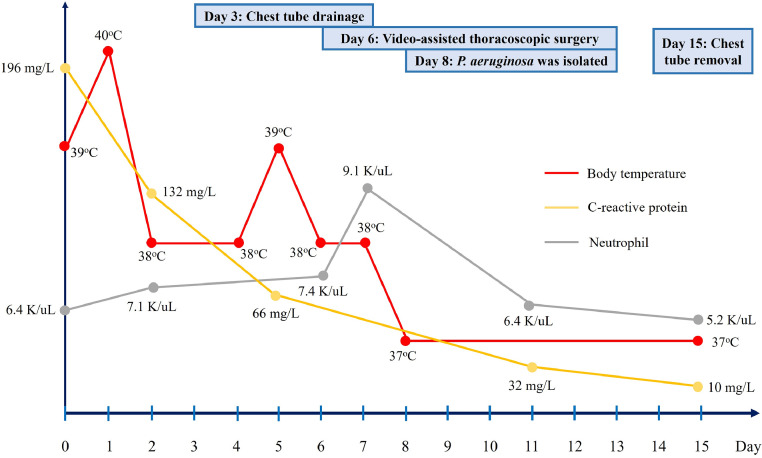
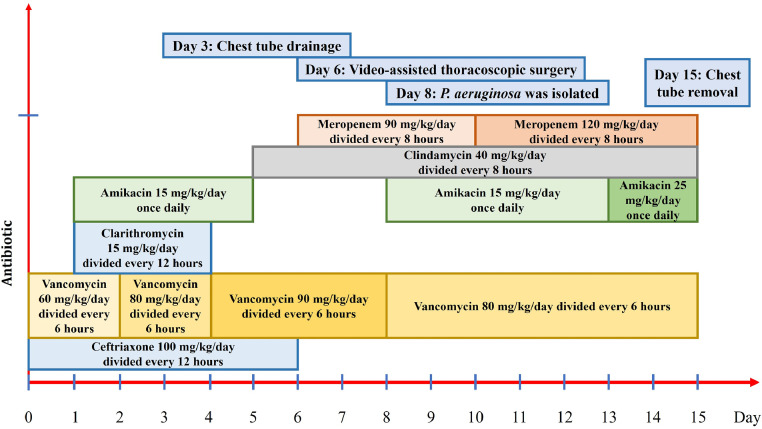
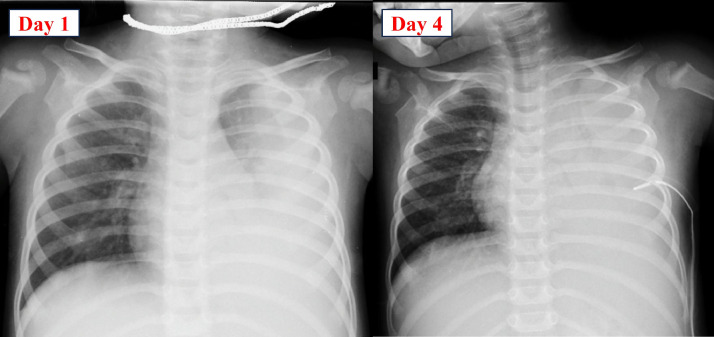
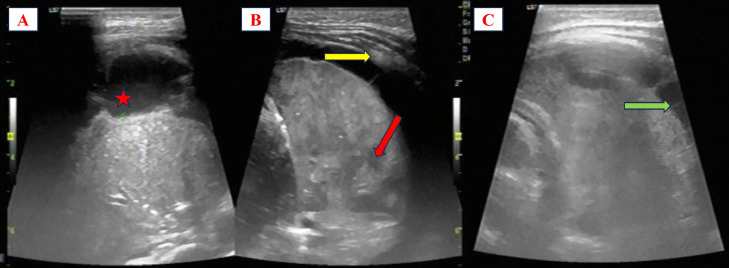
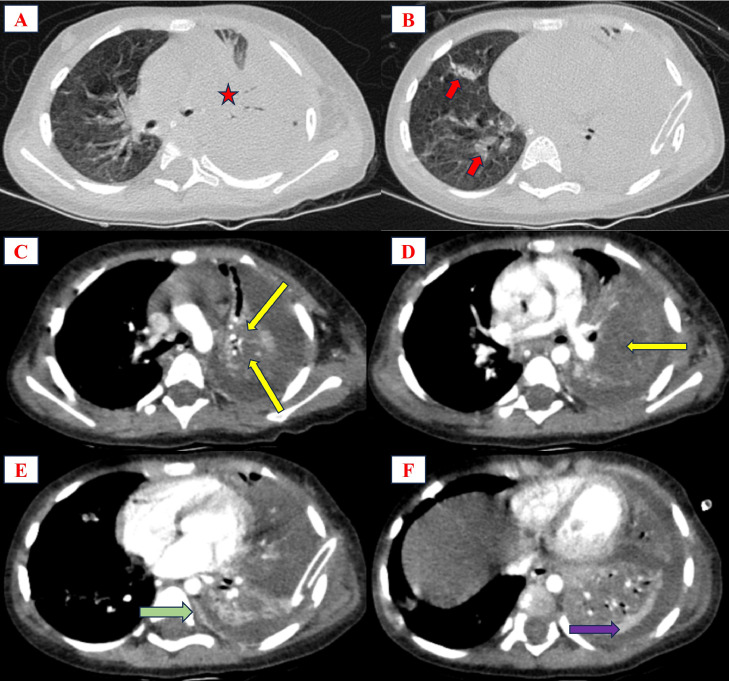
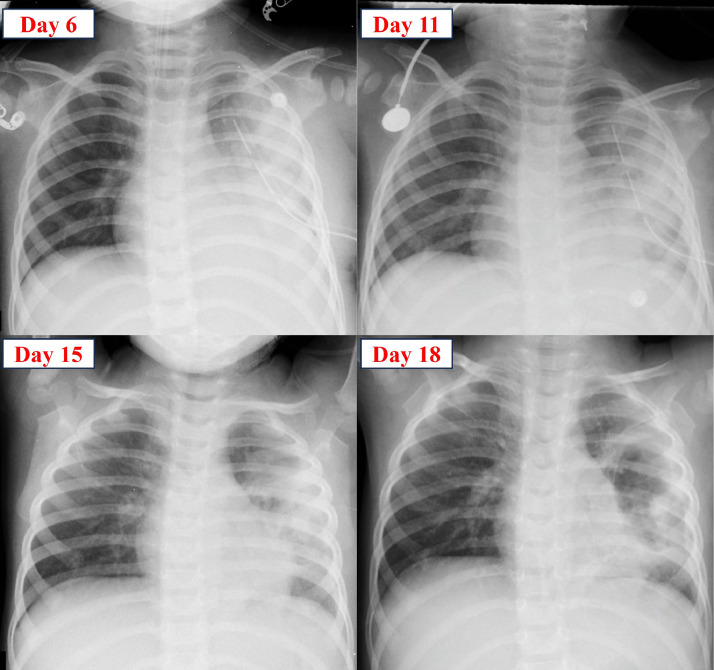
Necrotizing pneumonia (NP) is characterized by destruction of pulmonary tissue, resulting in multiple thin-walled cavities. There are limited reports on NP and parapneumonic effusion cases in children associated with Pseudomonas aeruginosa. Currently, there is no consensus regarding the optimal timing for video-assisted thoracoscopic surgery (VATS) following failure of chest tube placement and antibiotic treatment. A healthy 20-month-old child was hospitalized with symptoms of community-acquired pneumonia, progressing to severe NP and parapneumonic effusion. Despite receiving broad-spectrum antibiotics and chest tube placement on the third day of treatment, the condition continued to deteriorate, prompting VATS intervention on the sixth day. The presence of a "split pleural sign" and extensive lung necrosis on chest computed tomography contributed to initial treatment failure. Multidrug resistance P. aeruginosa was identified through nasal trachea aspiration specimens on the eighth day of treatment, leading to an adjustment in antibiotic therapy to high-dose meropenem and amikacin. Subsequently, the patient became afebrile, showed clinical improvement, and was discharged after 35 days of treatment. Through this case, we aim to emphasize an unusual pathogenic bacteria in the context of NP and the need for standardized surgical interventions in pediatric patients with NP.
Keywords: Necrotizing pneumonia; Pediatrics; Pseudomonas aeruginosa; VATS.
© 2024 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
Similar articles
-
Comparative analysis of chest tube thoracostomy and video-assisted thoracoscopic surgery in empyema and parapneumonic effusion associated with pneumonia in children.Surg Infect (Larchmt). 2008 Jun;9(3):317-23. doi: 10.1089/sur.2007.025. Surg Infect (Larchmt). 2008. PMID: 18570573
-
A Retrospective Chart Review of Pediatric Complicated Community-Acquired Pneumonia: An Experience in the Al Qassimi Women and Children Hospital.Cureus. 2022 Nov 5;14(11):e31119. doi: 10.7759/cureus.31119. eCollection 2022 Nov. Cureus. 2022. PMID: 36382327 Free PMC article.
-
Clinical outcome of urgent thoracoscopic surgery on complicated parapneumonic infection with short-term preoperative antibiotic usage.J Thorac Dis. 2025 Jan 24;17(1):357-368. doi: 10.21037/jtd-24-1331. Epub 2025 Jan 22. J Thorac Dis. 2025. PMID: 39975742 Free PMC article.
-
Current treatment of pediatric empyema.Semin Thorac Cardiovasc Surg. 2004 Fall;16(3):196-200. doi: 10.1053/j.semtcvs.2004.08.004. Semin Thorac Cardiovasc Surg. 2004. PMID: 15619185 Review.
-
Necrotizing pneumonia: an emerging problem in children?Pneumonia (Nathan). 2017 Jul 25;9:11. doi: 10.1186/s41479-017-0035-0. eCollection 2017. Pneumonia (Nathan). 2017. PMID: 28770121 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
