

Clinical Profile of Triple-Negative Breast Cancer: A Hospital-Based Study
- PMID: 38435145
- PMCID: PMC10907967
- DOI: 10.7759/cureus.53373
Clinical Profile of Triple-Negative Breast Cancer: A Hospital-Based Study
Abstract
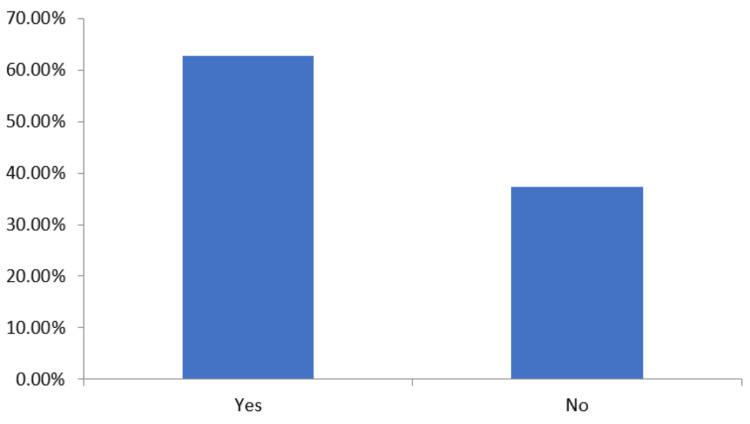
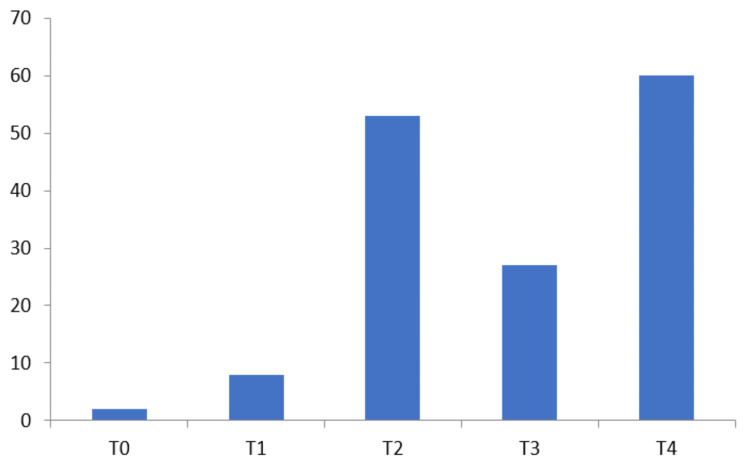
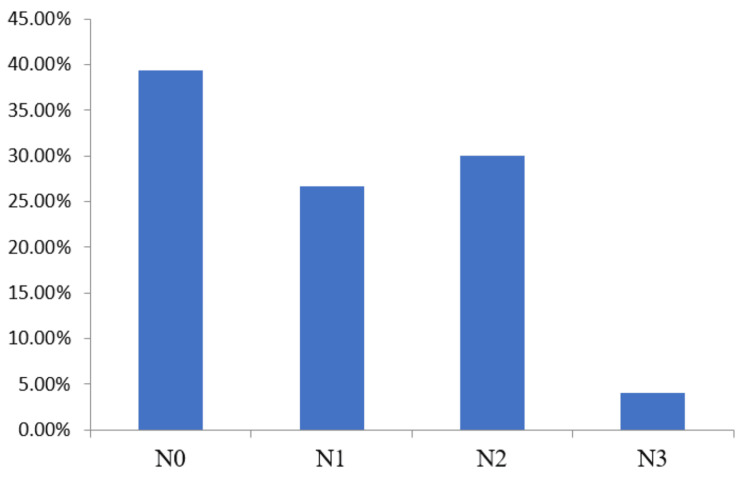
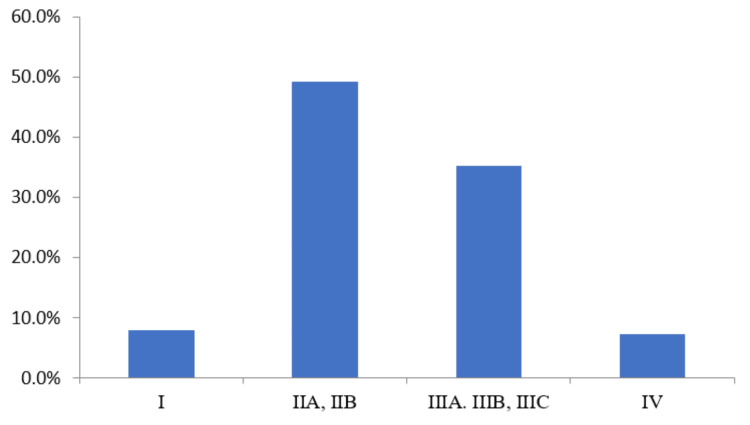
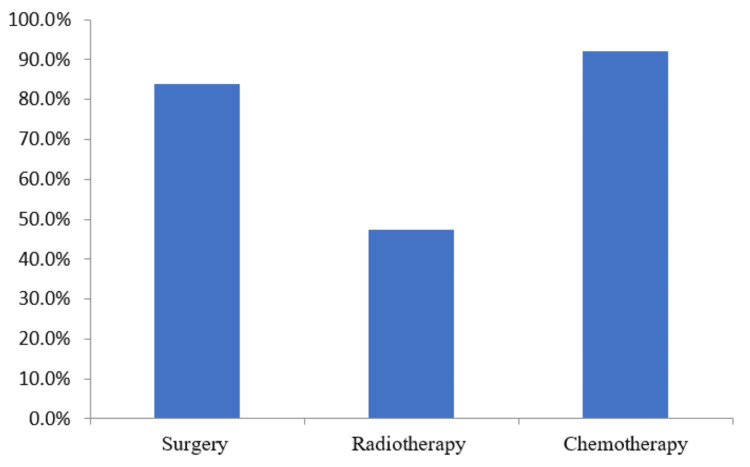
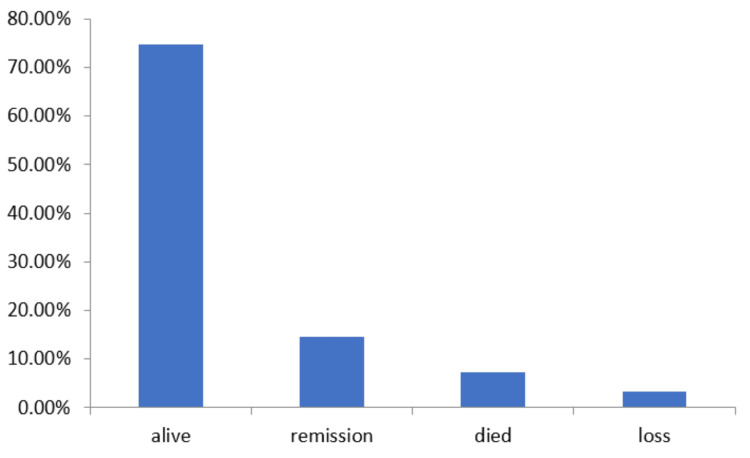
Introduction Triple-negative breast cancer (TNBC) is a new concept and an important area of investigation. In Western country's literature, different studies reported on TNBC and all indicated the poor prognostic aspect of this molecular subtype over other types of breast cancer. However, there is a scarcity of comprehensive data from India. Hence, the present study was carried out to look at the epidemiological and clinical characteristics of TNBC in the Indian population. Methods The present study was performed between January 2020 and June 2021 at a tertiary care hospital in Eastern India. A total of 150 patients with TNBC were enrolled in the study. The epidemiological and clinical features of enrolled patients were collected and reviewed. Results The median age of patients at TNBC presentation was 45.53 years (24 to 74 years). The median tumor size was reported to be 5.32 cm. Of 150 patients, 94(62.67%) showed enlarged lymph nodes and 56 (37.33%) patients had no lymph node enlargement. In the present study, 85 (56.67%) patients were in the pre/perimenopausal stage at presentation, whereas 65 (43.33%) patients were in the postmenopausal stage. Upon evaluating the spread of TNBC, it was observed that a maximum of patients 60 (40%) were at the T4 stage and 56 (37.33%) at the N0 condition. The clinical staging of TNBC reported a maximum of 74 (49.33%) patients at the IIA, and IIB stages followed by 53 (35.33%) patients at the IIIA, IIIB, and IIIC stages and a minimum of 11 (7.33%) patients at stage IV. Only five (3.33%) patients were reported with a family history of breast cancer. Of all patients, 126 (84%) had detected early breast cancer thereby applicable for surgery at the time of presentation, whereas 71 (47.33%) patients were eligible for radiation therapy and 138 (92%) patients received chemotherapy. A total of 112 (74.67%) patients were found alive after 24 months of follow-up, 22 (4.67%) patients were observed with remission, and 11 (7.33%) patients died due to TNBC progression. During the course of follow-up, five (3.33%) patients were lost in the study. Conclusion TNBC is an aggressive malignancy that has a high risk of systemic relapses in the first two years after diagnosis. For more mature evidence on TNBC, longer follow-up of patients is necessary.
Keywords: breast cancer; chemotherapy; clinical profile; triple-negative breast cancer; tumor.
Copyright © 2024, Pankaj et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Epidemiological and clinical profile of triple negative breast cancer at a cancer hospital in North India.Indian J Med Paediatr Oncol. 2013 Apr;34(2):89-95. doi: 10.4103/0971-5851.116185. Indian J Med Paediatr Oncol. 2013. PMID: 24049294 Free PMC article.
-
Novel Insights Into the Epidemiological and Clinico-Pathological Profile of Triple-Negative Breast Cancer: Dissection of an Aggressive Variant.Cureus. 2024 Mar 13;16(3):e56124. doi: 10.7759/cureus.56124. eCollection 2024 Mar. Cureus. 2024. PMID: 38618474 Free PMC article.
-
(18)F-FDG-PET/CT for systemic staging of newly diagnosed triple-negative breast cancer.Eur J Nucl Med Mol Imaging. 2016 Oct;43(11):1937-44. doi: 10.1007/s00259-016-3402-9. Epub 2016 Apr 30. Eur J Nucl Med Mol Imaging. 2016. PMID: 27129866 Free PMC article.
-
Current strategy for triple-negative breast cancer: appropriate combination of surgery, radiation, and chemotherapy.Breast Cancer. 2011 Jul;18(3):165-73. doi: 10.1007/s12282-011-0254-9. Epub 2011 Feb 3. Breast Cancer. 2011. PMID: 21290263 Review.
-
Metaplastic Carcinoma of the Breast Is More Aggressive Than Triple-negative Breast Cancer: A Study From a Single Institution and Review of Literature.Clin Breast Cancer. 2017 Aug;17(5):382-391. doi: 10.1016/j.clbc.2017.04.009. Epub 2017 Apr 26. Clin Breast Cancer. 2017. PMID: 28529029 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources