

Integrative single-cell expression and functional studies unravels a sensitization to cytarabine-based chemotherapy through HIF pathway inhibition in AML leukemia stem cells
- PMID: 38435427
- PMCID: PMC10895904
- DOI: 10.1002/hem3.45
Integrative single-cell expression and functional studies unravels a sensitization to cytarabine-based chemotherapy through HIF pathway inhibition in AML leukemia stem cells
Abstract
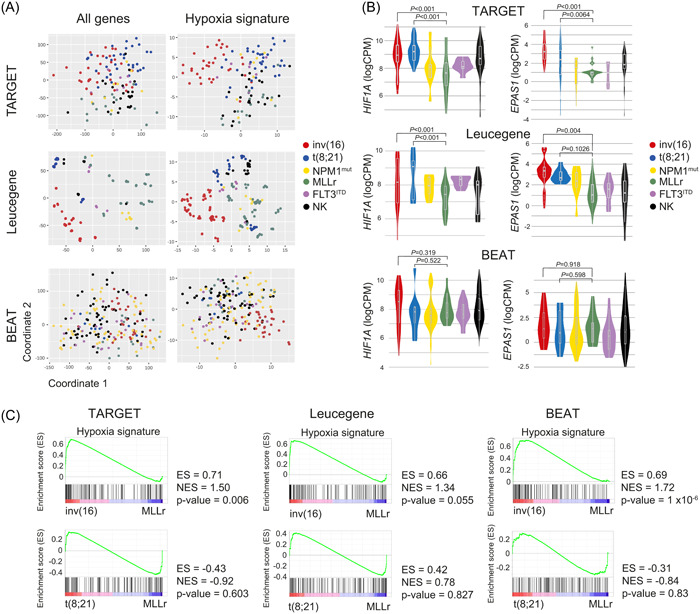
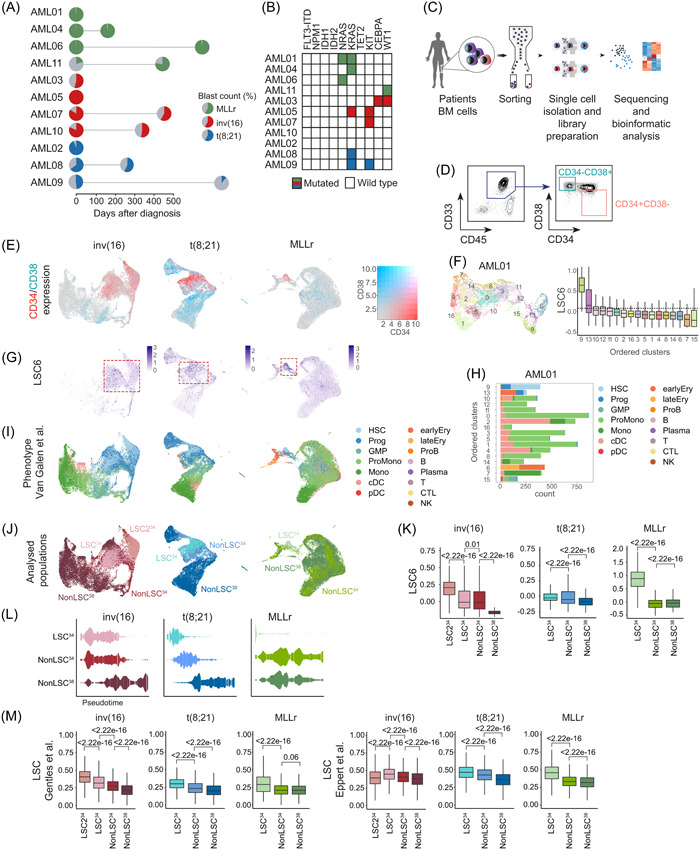
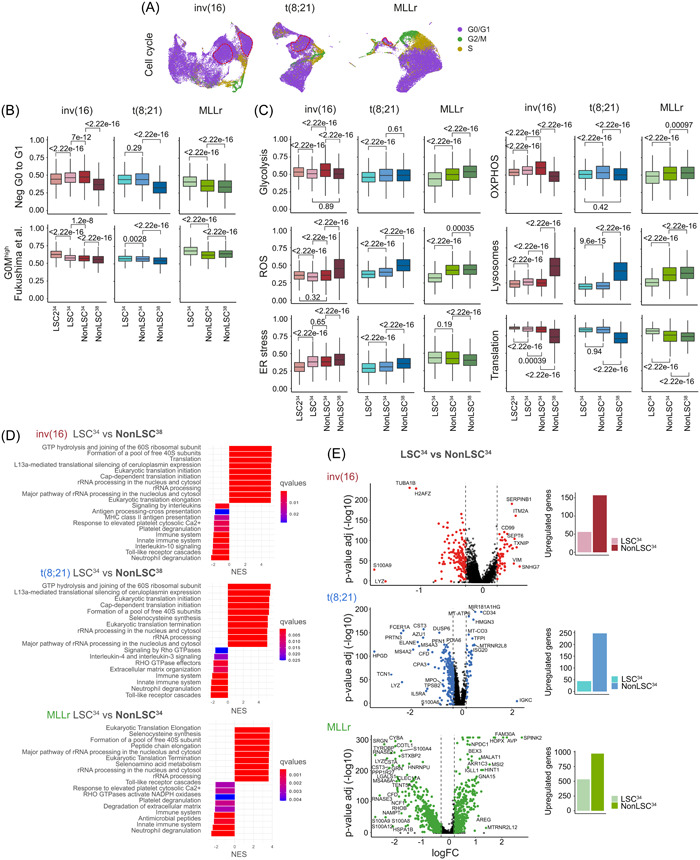
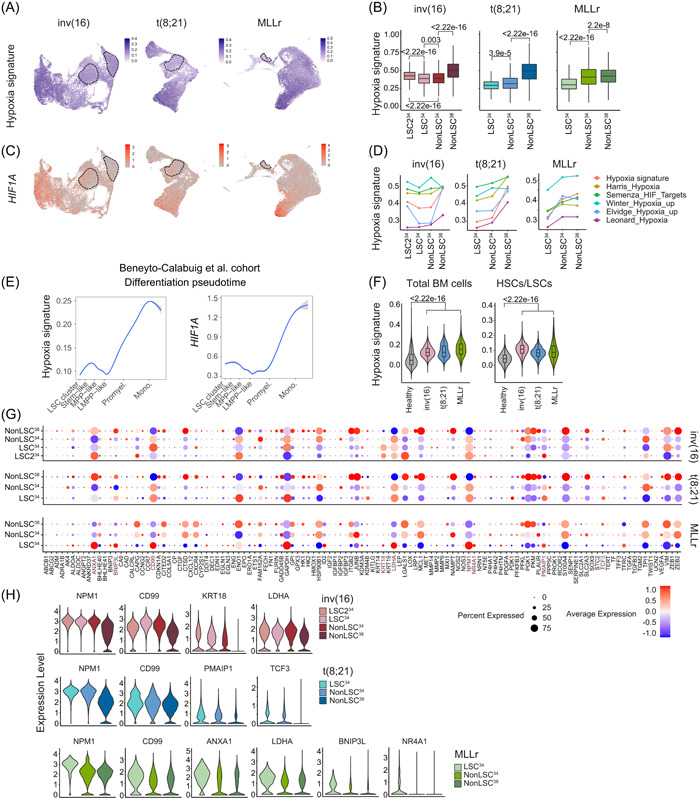
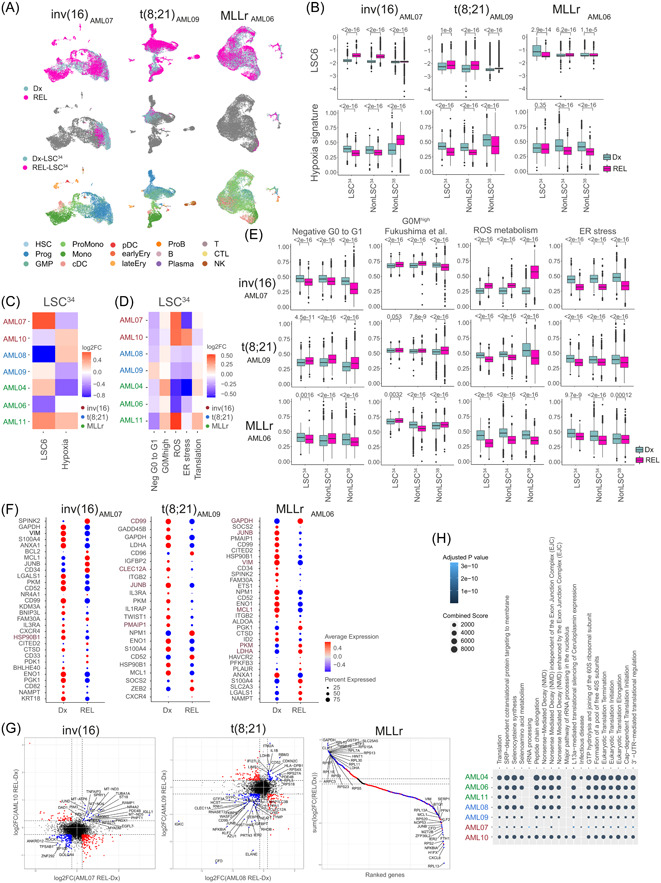
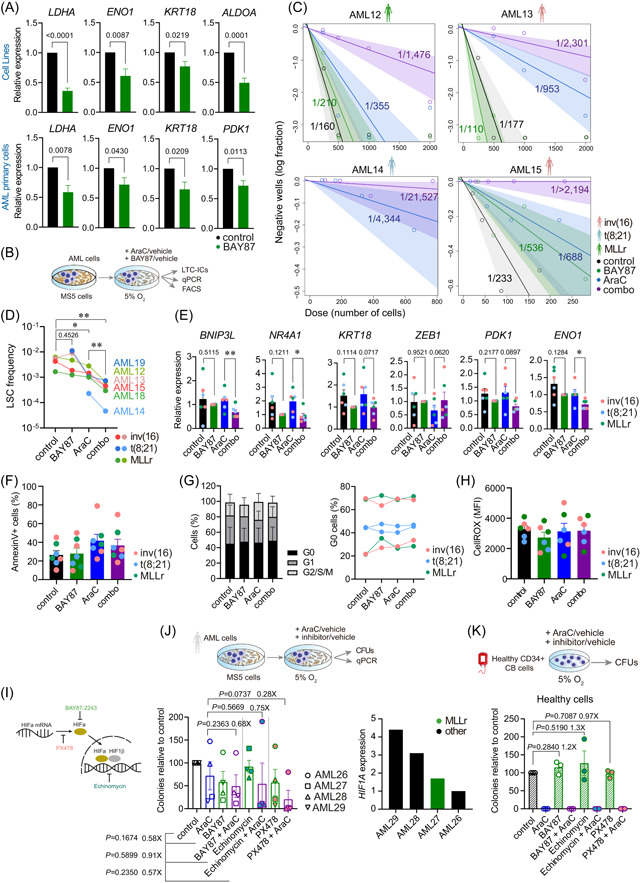
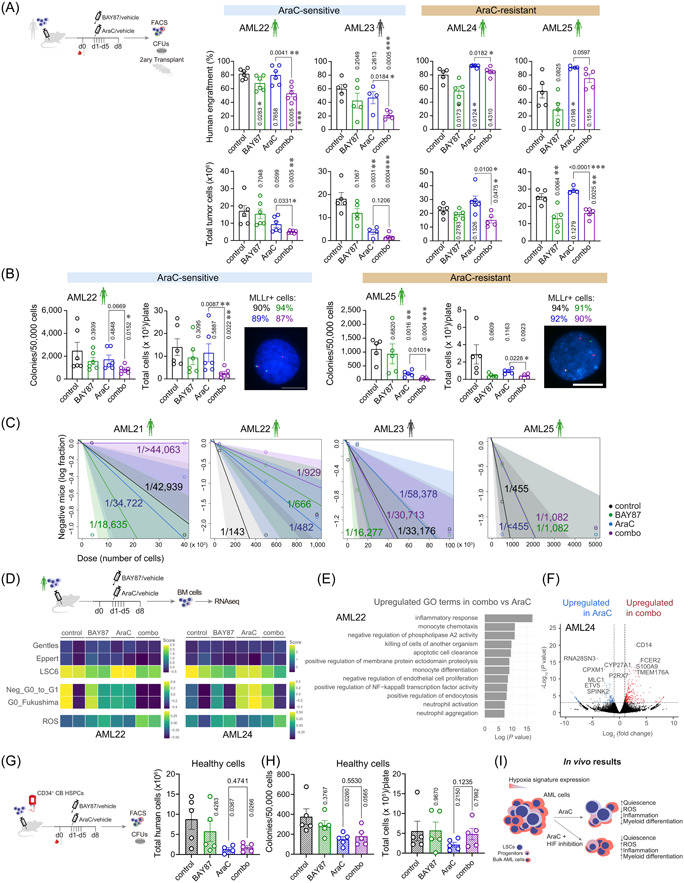
Relapse remains a major challenge in the clinical management of acute myeloid leukemia (AML) and is driven by rare therapy-resistant leukemia stem cells (LSCs) that reside in specific bone marrow niches. Hypoxia signaling maintains cells in a quiescent and metabolically relaxed state, desensitizing them to chemotherapy. This suggests the hypothesis that hypoxia contributes to the chemoresistance of AML-LSCs and may represent a therapeutic target to sensitize AML-LSCs to chemotherapy. Here, we identify HIFhigh and HIFlow specific AML subgroups (inv(16)/t(8;21) and MLLr, respectively) and provide a comprehensive single-cell expression atlas of 119,000 AML cells and AML-LSCs in paired diagnostic-relapse samples from these molecular subgroups. The HIF/hypoxia pathway signature is attenuated in AML-LSCs compared with more differentiated AML cells but is more expressed than in healthy hematopoietic cells. Importantly, chemical inhibition of HIF cooperates with standard-of-care chemotherapy to impair AML growth and to substantially eliminate AML-LSCs in vitro and in vivo. These findings support the HIF pathway in the stem cell-driven drug resistance of AML and unravel avenues for combinatorial targeted and chemotherapy-based approaches to specifically eliminate AML-LSCs.
© 2024 The Authors. HemaSphere published by John Wiley & Sons Ltd. on behalf of European Hematology Association.
Conflict of interest statement
Pablo Menéndez is the founder of the spin‐off OneChain Immunotherapeutics, which has no connection with the present research. The other authors declare no conflict of interest.
Figures
Comment in
-
From hypoxia single-cell gene signatures to HIF targeting of AML leukemic stem cells.Hemasphere. 2024 Mar 29;8(3):e59. doi: 10.1002/hem3.59. eCollection 2024 Mar. Hemasphere. 2024. PMID: 38560647 Free PMC article. No abstract available.
References
-
- Döhner H, Wei AH, Löwenberg B. Towards precision medicine for AML. Nat Rev Clin Oncol. 2021;18(9):577‐590. - PubMed
-
- Bonnet D, Dick JE. Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med. 1997;3(7):730‐737. - PubMed
-
- Shlush LI, Mitchell A, Heisler L, et al. Tracing the origins of relapse in acute myeloid leukaemia to stem cells. Nature. 2017;547(7661):104‐108. - PubMed