

Sentinel Node Mapping in Ovarian Tumors: A Study Using Lymphoscintigraphy and SPECT/CT
- PMID: 38435483
- PMCID: PMC10907102
- DOI: 10.1155/2024/5453692
Sentinel Node Mapping in Ovarian Tumors: A Study Using Lymphoscintigraphy and SPECT/CT
Abstract
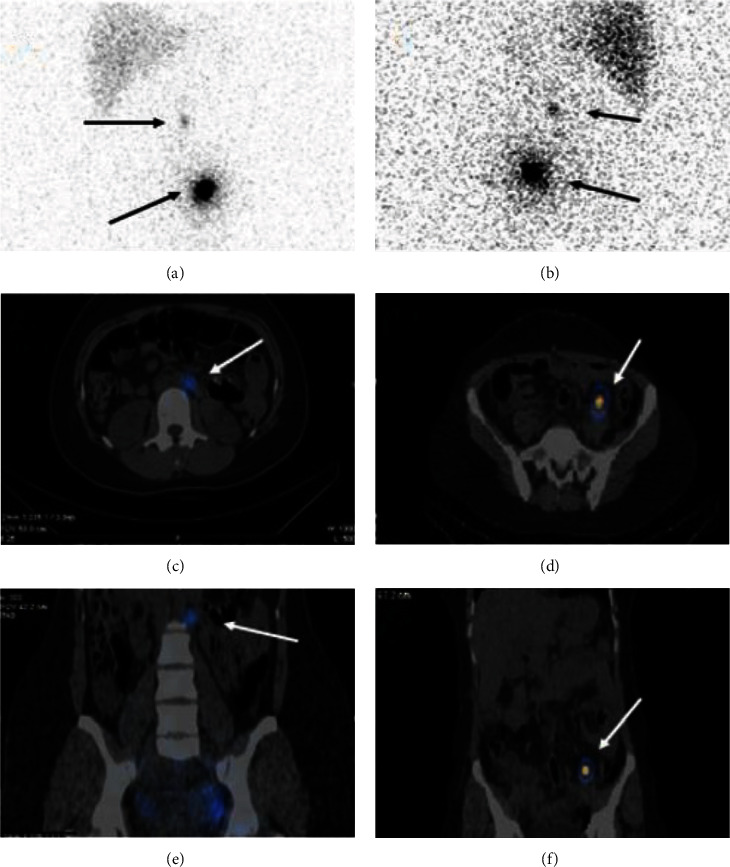
Purpose: Ovarian cancer in the early stage requires a complete surgical staging, including radical lymphadenectomy, implying subsequent risk of morbidity and complications. Sentinel lymph node (SLN) mapping is a procedure that attempts to reduce radical lymphadenectomy-related complications and morbidities. Our study evaluates the feasibility of SLN mapping in patients with ovarian tumors by the use of intraoperative Technetium-99m-Phytate (Tc-99m-Phytate) and postoperative lymphoscintigraphy using tomographic (single-photon emission computed tomography/computed tomography (SPECT/CT)) acquisition.
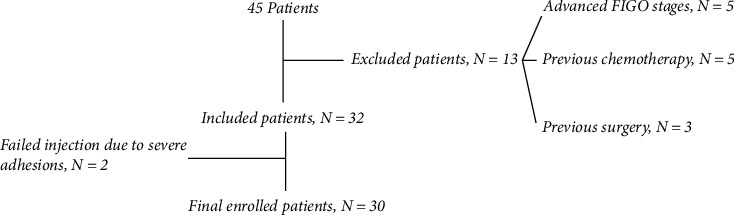
Materials and methods: Thirty-two patients with ovarian mass participated in this study. Intraoperative injection of the radiopharmaceutical was performed just after laparotomy and before the removal of tumor in utero-ovarian and suspensory ligaments of the ovary just beneath the peritoneum. Subsequently, pelvic and para-aortic lymphadenectomy was performed for malignant masses, and the presence of tumor in the lymph nodes was assessed through histopathological examination. Conversely, lymphadenectomy was not performed in patients with benign lesions or borderline ovarian tumors. Lymphoscintigraphy was performed within 24 hr using tomographic acquisition (SPECT/CT) of the abdomen and pelvis.
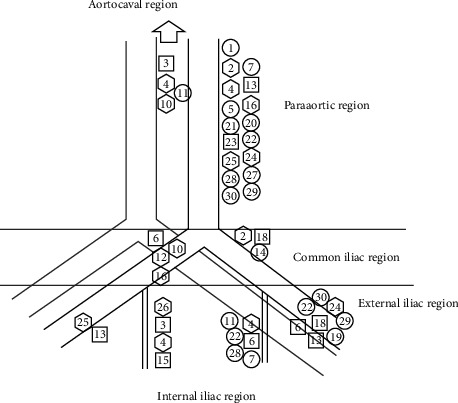
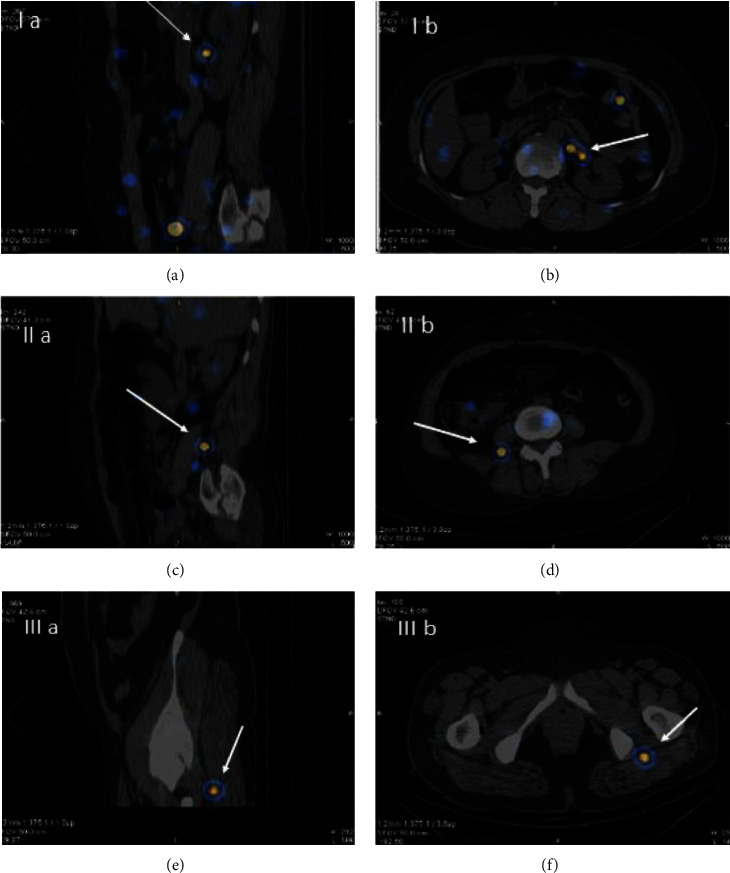
Results: Final pathological examination showed 19 patients with benign pathology, 5 with borderline tumors, and 6 with malignant ovarian tumors. SPECT/CT identified SLNs in para-aortic-only areas in 6 (20%), pelvic/para-aortic areas in 14 (47%), and pelvic-only areas in 7 (23%) cases. Notably, additional unusual SLN locations were revealed in perirenal, intergluteal, and posterior to psoas muscle regions in three patients. We were not able to calculate the false negative rate due to the absence of patients with involved lymph nodes.
Conclusion: SLN mapping using intraoperative injection of radiotracers is safe and feasible. Larger studies with more malignant cases are needed to better evaluate the sensitivity of this method for lymphatic staging of ovarian malignancies.
Copyright © 2024 Saeideh Ataei Nakhaei et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Lymphatic mapping and sentinel node biopsy in ovarian tumors: a study using intra-operative Tc-99m-Phytate and lymphoscintigraphy imaging.J Ovarian Res. 2016 Sep 7;9(1):55. doi: 10.1186/s13048-016-0265-4. J Ovarian Res. 2016. PMID: 27604260 Free PMC article.
-
Isthmocervical labelling and SPECT/CT for optimized sentinel detection in endometrial cancer: technique, experience and results.Gynecol Oncol. 2014 Aug;134(2):287-92. doi: 10.1016/j.ygyno.2014.05.001. Epub 2014 May 10. Gynecol Oncol. 2014. PMID: 24823647
-
The Added Value of SPECT/CT in Sentinel Lymph Nodes Mapping for Endometrial Carcinoma.Ann Surg Oncol. 2016 Feb;23(2):450-5. doi: 10.1245/s10434-015-4877-5. Epub 2015 Oct 5. Ann Surg Oncol. 2016. PMID: 26438438
-
Sentinel node approach in prostate cancer.Rev Esp Med Nucl Imagen Mol. 2015 Nov-Dec;34(6):358-71. doi: 10.1016/j.remn.2015.07.007. Epub 2015 Sep 29. Rev Esp Med Nucl Imagen Mol. 2015. PMID: 26391573 Review. English, Spanish.
-
Feasibility of sentinel lymph node mapping in ovarian tumors: A systematic review and meta-analysis of the literature.Front Med (Lausanne). 2022 Aug 1;9:950717. doi: 10.3389/fmed.2022.950717. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35979203 Free PMC article.
Cited by
-
Editorial: Sentinel lymph node mapping: current applications and future perspectives.Front Med (Lausanne). 2024 May 21;11:1422549. doi: 10.3389/fmed.2024.1422549. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38841580 Free PMC article. No abstract available.
-
Future of sentinel node biopsy in ovarian cancer.Curr Opin Oncol. 2024 Sep 1;36(5):412-417. doi: 10.1097/CCO.0000000000001058. Epub 2024 Jul 16. Curr Opin Oncol. 2024. PMID: 39016276 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
