

Effect of opioid-free versus opioid-based strategies during multimodal anaesthesia on postoperative morphine consumption after bariatric surgery: a randomised double-blind clinical trial
- PMID: 38435809
- PMCID: PMC10906147
- DOI: 10.1016/j.bjao.2024.100263
Effect of opioid-free versus opioid-based strategies during multimodal anaesthesia on postoperative morphine consumption after bariatric surgery: a randomised double-blind clinical trial
Abstract
Background: The efficacy and safety of opioid-free anaesthesia during bariatric surgery remain debated, particularly when administering multimodal analgesia. As multimodal analgesia has become the standard of care in many centres, we aimed to determine if such a strategy coupled with either dexmedetomidine (opioid-free anaesthesia) or remifentanil with a morphine transition (opioid-based anaesthesia), would reduce postoperative morphine requirements and opioid-related adverse events.
Methods: In this prospective double-blind study, 172 class III obese patients having laparoscopic gastric bypass surgery were randomly allocated to receive either sevoflurane-dexmedetomidine anaesthesia with a continuous infusion of lidocaine and ketamine (opioid-free group) or sevoflurane-remifentanil anaesthesia with a morphine transition (opioid-based group). Both groups received at anaesthesia induction a bolus of magnesium, lidocaine, ketamine, paracetamol, diclofenac, and dexamethasone. The primary outcome was 24-h postoperative morphine consumption. Secondary outcomes included postoperative quality of recovery (QoR40), incidence of hypoxaemia, bradycardia, and postoperative nausea and vomiting (PONV).
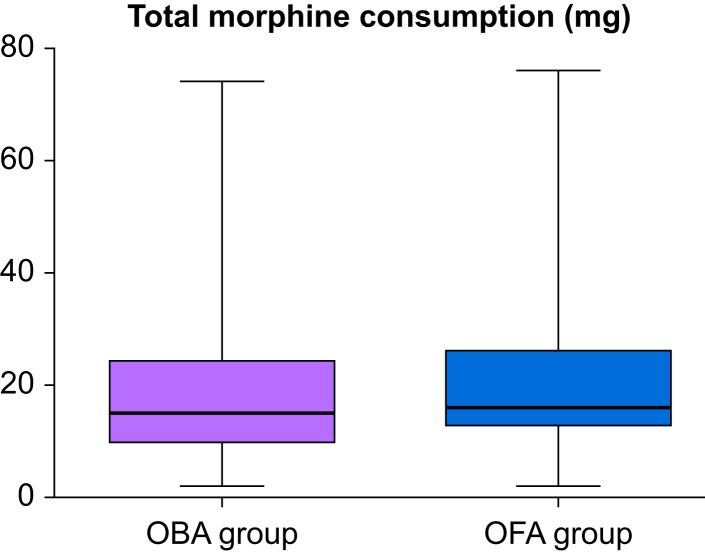
Results: Eighty-six patients were recruited in each group (predominantly women, 70% had obstructive sleep apnoea). There was no significant difference in postoperative morphine consumption (median [inter-quartile range]: 16 [13-26] vs 15 [10-24] mg, P=0.183). The QoR40 up to postoperative day 30 did not differ between groups, but PONV was less frequent in the opioid-free group (37% vs 59%, P=0.005). Hypoxaemia and bradycardia were not different between groups.
Conclusions: During bariatric surgery, a multimodal opioid-free anaesthesia technique did not decrease postoperative morphine consumption when compared with a multimodal opioid-based strategy. Quality of recovery did not differ between groups although the incidence of PONV was less in the opioid-free group.
Clinical trial registration: NCT05004519.
Keywords: dexmedetomidine; enhanced recovery after surgery; hypoxaemia; nausea; nociception; pain; remifentanil; vomiting.
© 2024 The Author(s).
Figures



References
-
- Dinges H.C., Otto S., Stay D.K., et al. Side effect rates of opioids in equianalgesic doses via intravenous patient-controlled analgesia: a systematic review and network meta-analysis. Anesth Analg. 2019;129:1153–1162. - PubMed
-
- de Boer H.D., Detriche O., Forget P. Opioid-related side effects: postoperative ileus, urinary retention, nausea and vomiting, and shivering. A review of the literature. Best Pract Res Clin Anaesthesiol. 2017;31:499–504. - PubMed
-
- Lavand'homme P., Steyaert A. Opioid-free anesthesia opioid side effects: tolerance and hyperalgesia. Best Pract Res Clin Anaesthesiol. 2017;31:487–498. - PubMed
-
- Ingrande J., Lemmens H.J. Dose adjustment of anaesthetics in the morbidly obese. Br J Anaesth. 2010;105(Suppl 1):i16–i23. - PubMed
-
- Sin J.C.K., Tabah A., Mjj Campher, Laupland K.B., Eley V.A. The effect of dexmedetomidine on postanesthesia care unit discharge and recovery: a systematic review and meta-analysis. Anesth Analg. 2022;134:1229–1244. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
