

Extra-pulmonary Cutaneous Sarcoidosis Presenting With Granulomatous Cranial Lesions and Cardiac Complications: A Case Report
- PMID: 38435864
- PMCID: PMC10905987
- DOI: 10.7759/cureus.53290
Extra-pulmonary Cutaneous Sarcoidosis Presenting With Granulomatous Cranial Lesions and Cardiac Complications: A Case Report
Abstract
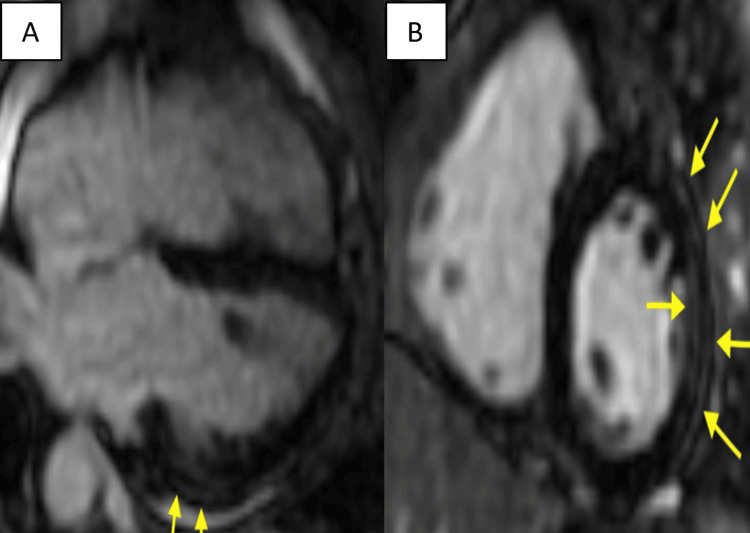
Sarcoidosis is a non-caseating granulomatous disorder affecting multiple organs. Although the lungs are the most common site of presentation, extra-pulmonary manifestations involving the skin and heart can occur. Sarcoidosis affecting skull bone is uncommon and involvement of skin, heart, and skull bone all together, without pulmonary manifestations, is extremely rare. We report a 63-year-old Caucasian woman with a past history of cutaneous sarcoidosis and granulomatous skull bone lesions who presented with recurrent syncope. An ambulatory cardiac monitor detected intermittent high-grade atrioventricular block and cardiac MRI confirmed the diagnosis of cardiac sarcoidosis. This case represents an extremely unique journey of sarcoidosis and suggests potential consideration for cardiac sarcoidosis screening in patients with a history of extra-cardiac manifestations.
Keywords: complications of sarcoidosis; cutaneous sarcoidosis; extra-pulmonary manifestations; granulomatous disorder; granulomatous skull bone lesions; high-grade atrioventricular block; multisystemic sarcoidosis.
Copyright © 2024, Vu et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- Clinical characteristics of patients in a case control study of sarcoidosis. Baughman RP, Teirstein AS, Judson MA, et al. Am J Respir Crit Care Med. 2001;164:1885–1889. - PubMed
-
- Biomarkers in the diagnosis and prognosis of sarcoidosis: current use and future prospects. Kraaijvanger R, Janssen Bonás M, Vorselaars AD, Veltkamp M. https://doi.org/10.3389/fimmu.2020.01443. Front Immunol. 2020;11:1443. - PMC - PubMed
-
- Sarcoidosis in America. Analysis based on health care use. Baughman RP, Field S, Costabel U, et al. https://doi.org/10.1513/annalsats.201511-760oc. Ann Am Thorac Soc. 2016;13:1244–1252. - PubMed
-
- Sarcoidosis--scientific progress and clinical challenges. Chen ES, Moller DR. Nat Rev Rheumatol. 2011;7:457–467. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous