

Chronic Inflammatory Demyelinating Polyradiculoneuropathy: Current Therapeutic Approaches and Future Outlooks
- PMID: 38435981
- PMCID: PMC10906673
- DOI: 10.2147/ITT.S388151
Chronic Inflammatory Demyelinating Polyradiculoneuropathy: Current Therapeutic Approaches and Future Outlooks
Abstract
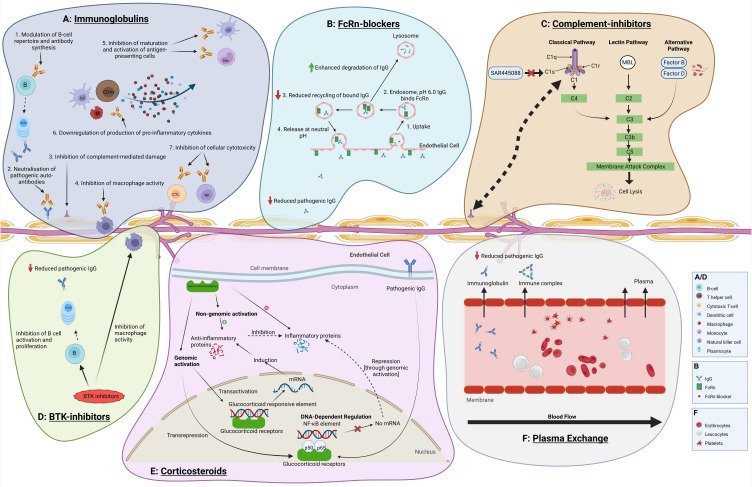
Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) is a treatable autoimmune disorder, for which different treatment options are available. Current first-line evidence-based therapies for CIDP include intravenous and subcutaneous immunoglobulins, corticosteroids and plasma exchanges. Despite lack of evidence, cyclophosphamide, rituximab and mycophenolate mofetil are commonly used in circumstances of refractoriness and, more debatably, of perceived overdependence on first-line therapies. Rituximab is currently the object of a randomized controlled trial for CIDP. Based on case series, and although rarely considered, haematopoietic autologous stem cell transplants may be effective in refractory disease, with low mortality and high remission rates. A new therapeutic option has appeared with efgartigimod, a neonatal Fc receptor blocker, recently shown to significantly lower relapse rate versus placebo, after withdrawal from previous immunotherapy. Other neonatal Fc receptor blockers, nipocalimab and batoclimab, are under study. The C1 complement-inhibitor SAR445088, acting in the proximal portion of the classical complement system, is currently the subject of a new study in treatment-responsive, refractory and treatment-naïve subjects. Finally, Bruton Tyrosine Kinase inhibitors, which exert anti-B cell effects, may represent another future research avenue. The widening of the therapeutic armamentarium enhances the need for improved evaluation of treatment effects and reliable biomarkers in CIDP.
Keywords: CIDP; corticosteroids; efgartigimod; immunoglobulins; plasma exchange.
© 2024 Rajabally.
Conflict of interest statement
YAR has received speaker/consultancy honoraria from Takeda, LFB, Polyneuron, Argenx, Janssen, Sanofi and Dianthus; educational support and research grants from LFB; educational support from CSL Behring, all outside the submitted work.
Figures
Similar articles
-
Therapeutic Monoclonal Antibody Therapies in Chronic Autoimmune Demyelinating Neuropathies.Neurotherapeutics. 2022 Apr;19(3):874-884. doi: 10.1007/s13311-022-01222-x. Epub 2022 Mar 28. Neurotherapeutics. 2022. PMID: 35349079 Free PMC article. Review.
-
Unconventional treatments for chronic inflammatory demyelinating polyneuropathy.Neurodegener Dis Manag. 2017 Oct;7(5):331-342. doi: 10.2217/nmt-2017-0017. Epub 2017 Oct 18. Neurodegener Dis Manag. 2017. PMID: 29043889 Review.
-
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP): Current Therapies and Future Approaches.Curr Pharm Des. 2022;28(11):854-862. doi: 10.2174/1381612828666220325102840. Curr Pharm Des. 2022. PMID: 35339172 Review.
-
An innovative phase 2 proof-of-concept trial design to evaluate SAR445088, a monoclonal antibody targeting complement C1s in chronic inflammatory demyelinating polyneuropathy.J Peripher Nerv Syst. 2023 Jun;28(2):276-285. doi: 10.1111/jns.12551. Epub 2023 May 31. J Peripher Nerv Syst. 2023. PMID: 37119056 Clinical Trial.
-
Newer therapeutic options for chronic inflammatory demyelinating polyradiculoneuropathy.Drugs. 2009 May 29;69(8):987-1001. doi: 10.2165/00003495-200969080-00004. Drugs. 2009. PMID: 19496628 Review.
Cited by
-
A pathophysiological and mechanistic review of chronic inflammatory demyelinating polyradiculoneuropathy therapy.Front Immunol. 2025 Apr 14;16:1575464. doi: 10.3389/fimmu.2025.1575464. eCollection 2025. Front Immunol. 2025. PMID: 40297573 Free PMC article. Review.
-
Efficacy and Safety of Rescue Treatment with Plasma Exchange in Patients with Acute Inflammatory Neurological Disorders: A Single Center Experience.Neurol Int. 2024 Jul 10;16(4):761-775. doi: 10.3390/neurolint16040056. Neurol Int. 2024. PMID: 39051217 Free PMC article.
-
Brazilian Academy of Neurology recommendations for diagnosis, management, and treatment of chronic inflammatory demyelinating polyradiculoneuropathy (CIDP).Arq Neuropsiquiatr. 2025 Jul;83(7):1-19. doi: 10.1055/s-0045-1809884. Epub 2025 Jul 28. Arq Neuropsiquiatr. 2025. PMID: 40720971 Free PMC article.
References
-
- Van den Bergh PYK, van Doorn PA, Hadden RDM, et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: report of a joint Task Force-Second revision. Eur J Neurol. 2021;28(11):3556–3583. doi:10.1111/ene.14959 - DOI - PubMed
-
- Van den Bergh PY, Hadden RD, Bouche P, et al. European Federation of Neurological Societies/Peripheral Nerve Society guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society - first revision. Eur J Neurol. 2010;17(3):356–363. doi:10.1111/j.1468-1331.2009.02930.x - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
