

Torsemide Versus Furosemide After Discharge in Patients Hospitalized With Heart Failure Across the Spectrum of Ejection Fraction: Findings From TRANSFORM-HF
- PMID: 38436075
- PMCID: PMC10950535
- DOI: 10.1161/CIRCHEARTFAILURE.123.011246
Torsemide Versus Furosemide After Discharge in Patients Hospitalized With Heart Failure Across the Spectrum of Ejection Fraction: Findings From TRANSFORM-HF
Abstract
Background: The TRANSFORM-HF trial (Torsemide Comparison With Furosemide for Management of Heart Failure) found no significant difference in all-cause mortality or hospitalization among patients randomized to a strategy of torsemide versus furosemide following a heart failure (HF) hospitalization. However, outcomes and responses to some therapies differ by left ventricular ejection fraction (LVEF). Thus, we sought to explore the effect of torsemide versus furosemide by baseline LVEF and to assess outcomes across LVEF groups.
Methods: We compared baseline patient characteristics and randomized treatment effects for various end points in TRANSFORM-HF stratified by LVEF: HF with reduced LVEF, ≤40% versus HF with mildly reduced LVEF, 41% to 49% versus HF with preserved LVEF, ≥50%. We also evaluated associations between LVEF and clinical outcomes. Study end points were all-cause mortality or hospitalization at 30 days and 12 months, total hospitalizations at 12 months, and change from baseline in Kansas City Cardiomyopathy Questionnaire clinical summary score.
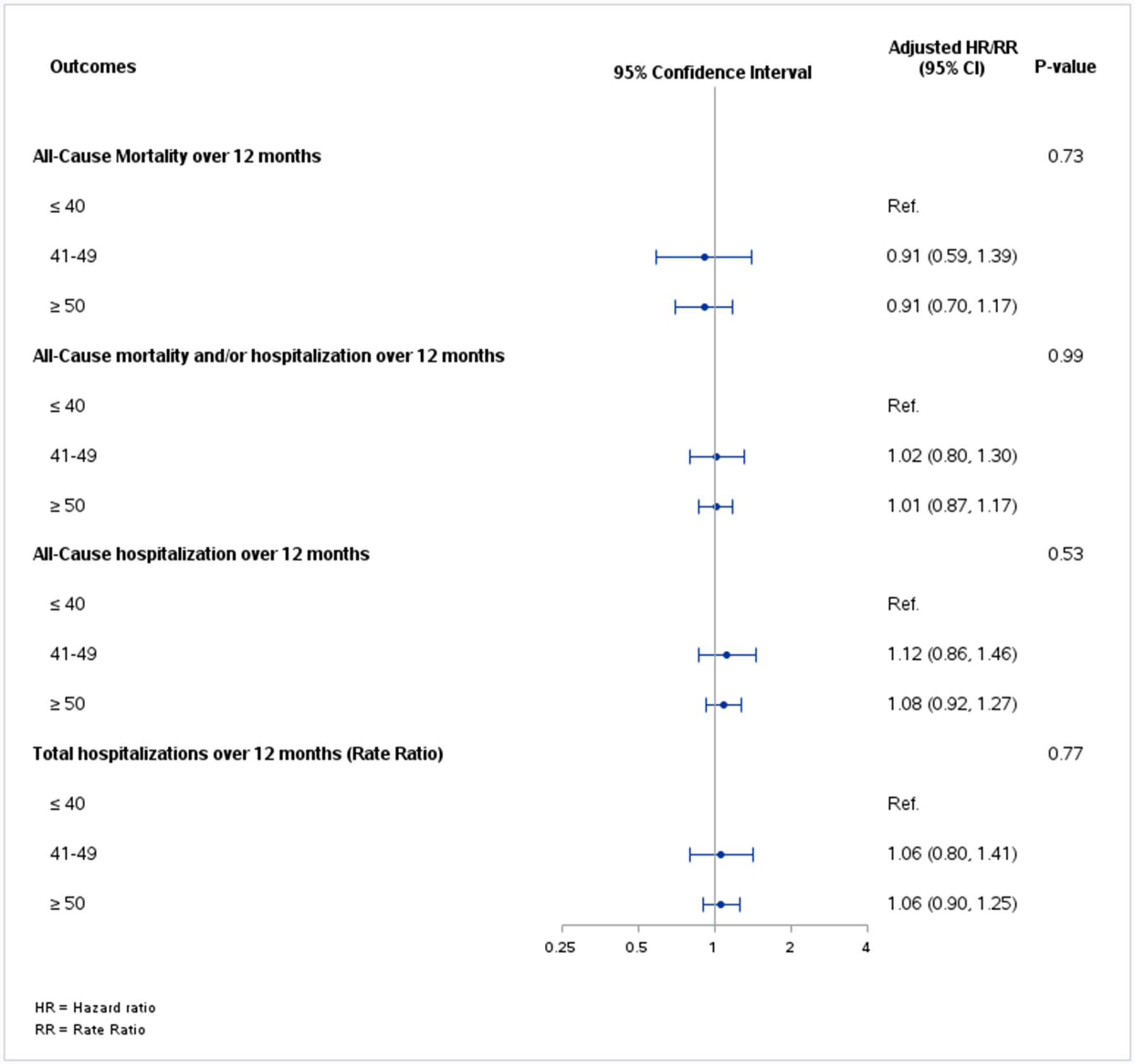
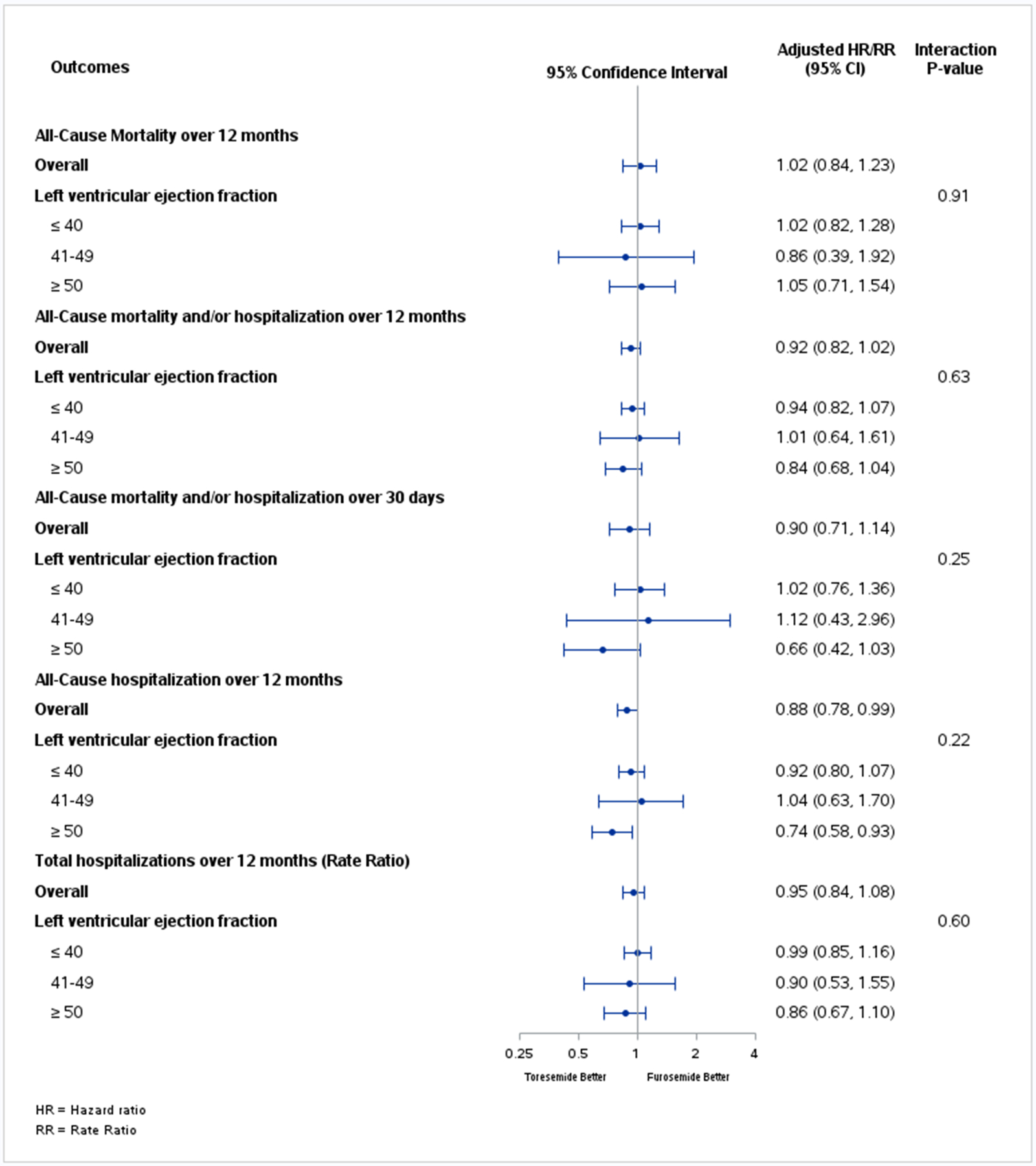
Results: Overall, 2635 patients (median 64 years, 36% female, 34% Black) had LVEF data. Compared with HF with reduced LVEF, patients with HF with mildly reduced LVEF and HF with preserved LVEF had a higher prevalence of comorbidities. After adjusting for covariates, there was no significant difference in risk of clinical outcomes across the LVEF groups (adjusted hazard ratio for 12-month all-cause mortality, 0.91 [95% CI, 0.59-1.39] for HF with mildly reduced LVEF versus HF with reduced LVEF and 0.91 [95% CI, 0.70-1.17] for HF with preserved LVEF versus HF with reduced LVEF; P=0.73). In addition, there was no significant difference between torsemide and furosemide (1) for mortality and hospitalization outcomes, irrespective of LVEF group and (2) in changes in Kansas City Cardiomyopathy Questionnaire clinical summary score in any LVEF subgroup.
Conclusions: Despite baseline demographic and clinical differences between LVEF cohorts in TRANSFORM-HF, there were no significant differences in the clinical end points with torsemide versus furosemide across the LVEF spectrum. There was a substantial risk for all-cause mortality and subsequent hospitalization independent of baseline LVEF.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT03296813.
Keywords: diuretics; hospitalization; mortality; quality of life.
Conflict of interest statement
Dr Greene has received research support from the Duke University Department of Medicine Chair’s Research Award, the American Heart Association (929502), the National Heart, Lung, and Blood Institute, Amgen, AstraZeneca, Bristol Myers Squibb, Cytokinetics, Merck, Novartis, Pfizer, and Sanofi; has served on advisory boards for Amgen, AstraZeneca, Boehringer Ingelheim/Lilly, Bristol Myers Squibb, Cytokinetics, Roche Diagnostics, and Sanofi; serves as a consultant for Amgen, Bayer, Bristol Myers Squibb, Boehringer Ingelheim/Lilly, CSL Vifor, Merck, PharmaIN, Roche Diagnostics, Sanofi, Tricog Health, Urovant Pharmaceuticals; and has received speaker fees from Boehringer Ingelheim, Cytokinetics, and Roche Diagnostics. Dr Anstrom has received research support from Merck, Bayer, Pfizer, National Institutes of Health, and the Patient-Centered Outcomes Research Institute. Dr Mentz receives research support and honoraria from Abbott, American Regent, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim/Eli Lilly, Boston Scientific, Cytokinetics, Fast BioMedical, Gilead, Innolife, Medtronic, Merck, Novartis, Pharmacosmos, Relypsa, Respicardia, Roche, Sanofi, Vifor, Windtree Therapeutics, and Zoll. All other authors report no conflicts.
Figures

Similar articles
-
Effect of Torsemide Versus Furosemide on Symptoms and Quality of Life Among Patients Hospitalized for Heart Failure: The TRANSFORM-HF Randomized Clinical Trial.Circulation. 2023 Jul 11;148(2):124-134. doi: 10.1161/CIRCULATIONAHA.123.064842. Epub 2023 May 22. Circulation. 2023. PMID: 37212600 Free PMC article. Clinical Trial.
-
Effect of Torsemide vs Furosemide After Discharge on All-Cause Mortality in Patients Hospitalized With Heart Failure: The TRANSFORM-HF Randomized Clinical Trial.JAMA. 2023 Jan 17;329(3):214-223. doi: 10.1001/jama.2022.23924. JAMA. 2023. PMID: 36648467 Free PMC article. Clinical Trial.
-
Torsemide vs Furosemide Among Patients With New-Onset vs Worsening Chronic Heart Failure: A Substudy of the TRANSFORM-HF Randomized Clinical Trial.JAMA Cardiol. 2024 Feb 1;9(2):182-188. doi: 10.1001/jamacardio.2023.4776. JAMA Cardiol. 2024. PMID: 37955908 Free PMC article. Clinical Trial.
-
Comparing torsemide versus furosemide in patients with heart failure: A meta-analysis.J Am Pharm Assoc (2003). 2019 May-Jun;59(3):432-438. doi: 10.1016/j.japh.2019.01.014. Epub 2019 Mar 4. J Am Pharm Assoc (2003). 2019. PMID: 30846351 Review.
-
Pragmatic Design of Randomized Clinical Trials for Heart Failure: Rationale and Design of the TRANSFORM-HF Trial.JACC Heart Fail. 2021 May;9(5):325-335. doi: 10.1016/j.jchf.2021.01.013. Epub 2021 Mar 10. JACC Heart Fail. 2021. PMID: 33714745 Free PMC article. Review.
Cited by
-
ANMCO position paper: diagnosis and treatment of heart failure with preserved systolic function.Eur Heart J Suppl. 2025 May 15;27(Suppl 5):v216-v246. doi: 10.1093/eurheartjsupp/suaf070. eCollection 2025 May. Eur Heart J Suppl. 2025. PMID: 40385467 Free PMC article.
-
Diuretics: a review of the pharmacology and effects on glucose homeostasis.Front Pharmacol. 2025 Mar 28;16:1513125. doi: 10.3389/fphar.2025.1513125. eCollection 2025. Front Pharmacol. 2025. PMID: 40223924 Free PMC article. Review.
References
-
- Vazir A, Kapelios CJ, Agaoglu E, Metra M, Lopatin Y, Seferovic P, Mullens W, Filippatos G, Rosano G, Coats AJS, et al. Decongestion Strategies in patients presenting with acutely decompensated heart failure: a worldwide survey among physicians. Eur J Heart Fail. 2023;25:1555–70. doi:10.1002/ejhf.2985 - DOI - PubMed
-
- Mentz RJ, Anstrom KJ, Eisenstein EL, Sapp S, Greene SJ, Morgan S, Testani JM, Harrington AH, Sachdev V, Ketema F, et al. Effect of Torsemide vs Furosemide After Discharge on All-Cause Mortality in Patients Hospitalized With Heart Failure. JAMA. 2023;329:214–23. doi:10.1001/jama.2022.23924 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
