

Biomarker cystatin B expression correlates with pathogenesis in cervical cancer
- PMID: 38436260
- PMCID: PMC10913530
- DOI: 10.1177/03000605241233959
Biomarker cystatin B expression correlates with pathogenesis in cervical cancer
Abstract
Objective: Cervical cancer (CC) is one of the most common gynecologic malignancies worldwide. Although rapid improvements have been made regarding its prevention and treatment, little is known about disease pathogenesis and the clinical relevance of reliable biomarkers. The present study evaluated the expression of cystatin B (CSTB) as a potential biomarker of CC.
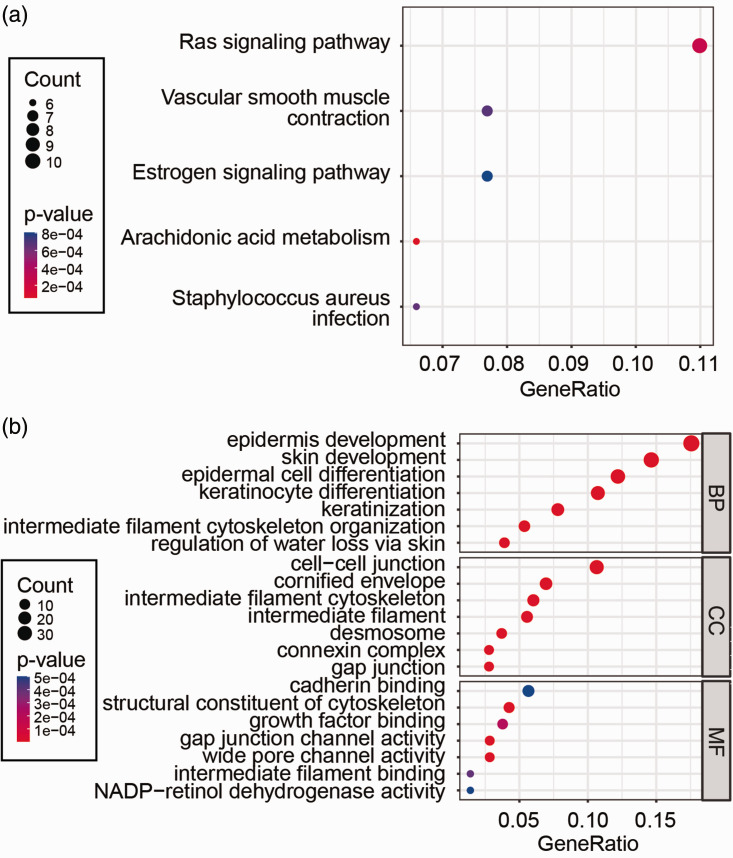
Methods: Tissue microarray analysis and immunohistochemical staining were performed to detect CSTB expression, while CSTB mRNA and protein expression levels of freshly isolated CC tissue were measured by quantitative real-time PCR and western blot, respectively. Bioinformatics were used to analyze the CSTB co-expression network and functional enrichments.
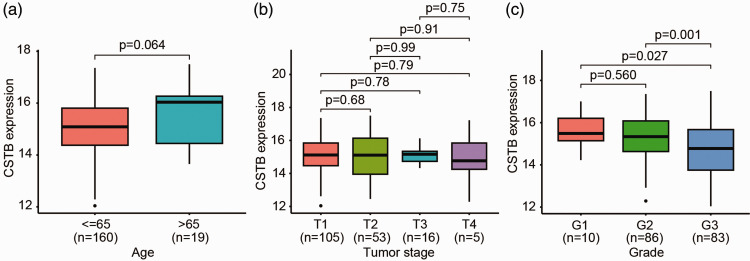
Results: We observed high CSTB mRNA and protein expression levels in CC tissues, which was confirmed by tissue microarray in a comparison with paired adjacent non-cancerous cervical tissue samples. CSTB gene enrichments and associations with co-expressed genes were also observed. Further analysis showed that elevated CSTB expression was associated with pathological progress in CC.
Conclusion: Our data demonstrate that CSTB has the potential to be used as a tissue biomarker with clinical value in patients with CC, which may aid the development of intervention strategies.
Keywords: Cystatin B; cervical cancer; lesion; pathological progress; tissue microarray; tumor.
Conflict of interest statement
Declaration of conflicting interestsThe authors declare that they have no competing interests.
Figures



Similar articles
-
Expression and epigenetic regulation of cystatin B in lung cancer and colorectal cancer.Pathol Res Pract. 2017 Dec;213(12):1568-1574. doi: 10.1016/j.prp.2017.06.007. Epub 2017 Jun 6. Pathol Res Pract. 2017. PMID: 29037838
-
Identification of cystatin B as a potential serum marker in hepatocellular carcinoma.Clin Cancer Res. 2008 Feb 15;14(4):1080-9. doi: 10.1158/1078-0432.CCR-07-1615. Clin Cancer Res. 2008. PMID: 18281540
-
Cystatin B is a progression marker of human epithelial ovarian tumors mediated by the TGF-β signaling pathway.Int J Oncol. 2014 Apr;44(4):1099-106. doi: 10.3892/ijo.2014.2261. Epub 2014 Jan 21. Int J Oncol. 2014. PMID: 24452274 Free PMC article.
-
Cystatin B increases autophagic flux by sustaining proteolytic activity of cathepsin B and fuels glycolysis in pancreatic cancer: CSTB orchestrates autophagy and glycolysis in PDAC.Clin Transl Med. 2022 Dec;12(12):e1126. doi: 10.1002/ctm2.1126. Clin Transl Med. 2022. PMID: 36495123 Free PMC article.
-
The epilepsy, the protease inhibitor and the dodecamer: progressive myoclonus epilepsy, cystatin b and a 12-mer repeat expansion.Cytogenet Genome Res. 2003;100(1-4):213-23. doi: 10.1159/000072857. Cytogenet Genome Res. 2003. PMID: 14526183 Review.
Cited by
-
Cystatin B Promotes the Proliferation, Migration, and Invasion of Intrahepatic Cholangiocarcinoma.Curr Oncol. 2025 Jan 21;32(2):56. doi: 10.3390/curroncol32020056. Curr Oncol. 2025. PMID: 39996856 Free PMC article.
-
Cathepsins and their role in gynecological cancers: Evidence from two-sample Mendelian randomization analysis.Medicine (Baltimore). 2025 Mar 7;104(10):e41653. doi: 10.1097/MD.0000000000041653. Medicine (Baltimore). 2025. PMID: 40068078 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, et al.. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209–249. DOI: 10.3322/caac.21660. - PubMed
-
- Saslow D, Solomon D, Lawson HW, et al.. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. Am J Clin Pathol 2012; 137: 516–542. DOI: 10.1309/AJCPTGD94EVRSJCG. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
