

Economic evaluations of assisted reproductive technologies in high-income countries: a systematic review
- PMID: 38438132
- PMCID: PMC11063548
- DOI: 10.1093/humrep/deae039
Economic evaluations of assisted reproductive technologies in high-income countries: a systematic review
Abstract
Study question: Which assited reproductive technology (ART) interventions in high-income countries are cost-effective and which are not?
Summary answer: Among all ART interventions assessed in economic evaluations, most high-cost interventions, including preimplantation genetic testing for aneuploidy (PGT-A) for a general population and ICSI for unexplained infertility, are unlikely to be cost-effective owing to minimal or no increase in effectiveness.
What is known already: Approaches to reduce costs in order to increase access have been identified as a research priority for future infertility research. There has been an increasing number of ART interventions implemented in routine clinical practice globally, before robust assessments of evidence on economic evaluations. The extent of clinical effectiveness of some studied comparisons has been evaluated in high-quality research, allowing more informative decision making around cost-effectiveness.
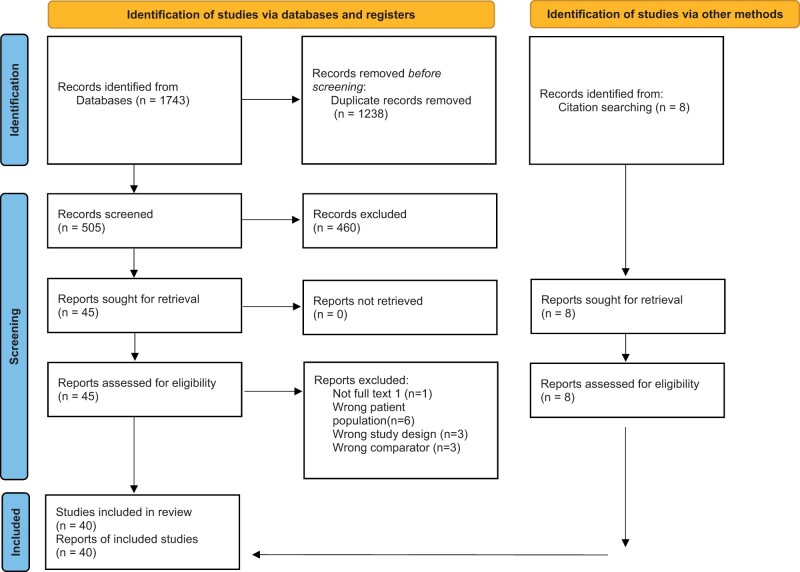
Study design, size, duration: We performed a systematic review and searched seven databases (MEDLINE, PUBMED, EMBASE, COCHRANE, ECONLIT, SCOPUS, and CINAHL) for studies examining ART interventions for infertility together with an economic evaluation component (cost-effectiveness, cost-benefit, cost-utility, or cost-minimization assessment), in high-income countries, published since January 2011. The last search was 22 June 2022.
Participants/materials, setting, methods: Two independent reviewers assessed publications and included those fulfilling the eligibility criteria. Studies were examined to assess the cost-effectiveness of the studied intervention, as well as the reporting quality of the study. The chosen outcome measure and payer perspective were also noted. Completeness of reporting was assessed against the Consolidated Health Economic Evaluation Reporting Standard. Results are presented and summarized based on the intervention studied.
Main results and the role of chance: The review included 40 studies which were conducted in 11 high-income countries. Most studies (n = 34) included a cost-effectiveness analysis. ART interventions included medication or strategies for controlled ovarian stimulation (n = 15), IVF (n = 9), PGT-A (n = 7), single embryo transfer (n = 5), ICSI (n = 3), and freeze-all embryo transfer (n = 1). Live birth was the mostly commonly reported primary outcome (n = 27), and quality-adjusted life years was reported in three studies. The health funder perspective was used in 85% (n = 34) of studies. None of the included studies measured patient preference for treatment. It remains uncertain whether PGT-A improves pregnancy rates compared to IVF cycles managed without PGT-A, and therefore cost-effectiveness could not be demonstrated for this intervention. Similarly, ICSI in non-male factor infertility appears not to be clinically effective compared to standard fertilization in an IVF cycle and is therefore not cost-effective. Interventions such as use of biosimilars or HMG for ovarian stimulation are cheaper but compromise clinical effectiveness.
Limitations, reasons for caution: Lack of both preference-based and standardized outcomes limits the comparability of results across studies. The selection of efficacy evidence offered for some interventions for economic evaluations is not always based on high-quality randomized trials and systematic reviews. In addition, there is insufficient knowledge of the willingness to pay thresholds of individuals and state funders for treatment of infertility. There is variable quality of reporting scores, which might increase uncertainty around the cost-effectiveness results.
Wider implications of the findings: Investment in strategies to help infertile people who utilize ART is justifiable at both personal and population levels. This systematic review may assist ART funders decide how to best invest to maximize the likelihood of delivery of a healthy child.
Study funding/competing interest(s): There was no funding for this study. E.C. and R.W. receive salary support from the National Health and Medical Research Council (NHMRC) through their fellowship scheme (EC GNT1159536, RW 2021/GNT2009767). M.D.-T. reports consulting fees from King Fahad Medical School. All other authors have no competing interests to declare.
Registration number: Prospero CRD42021261537.
Keywords: ART; IVF; assisted; cost-effectiveness; cost-utility; economic analysis; preimplantation genetic testing; reproductive techniques; systematic review.
© The Author(s) 2024. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Conflict of interest statement
M.D.-T. reports consulting fees from King Fahad Medical School. All other authors have no competing interests to declare.
Figures

Similar articles
-
International Committee for Monitoring Assisted Reproductive Technologies (ICMART): world report for cycles conducted in 2017-2018.Hum Reprod. 2025 Jun 1;40(6):1110-1126. doi: 10.1093/humrep/deaf049. Hum Reprod. 2025. PMID: 40239109
-
In vitro fertilization and multiple pregnancies: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(18):1-63. Epub 2006 Oct 1. Ont Health Technol Assess Ser. 2006. PMID: 23074488 Free PMC article.
-
Preimplantation genetic testing for aneuploidy by microarray analysis of polar bodies in advanced maternal age: a randomized clinical trial.Hum Reprod. 2018 Sep 1;33(9):1767-1776. doi: 10.1093/humrep/dey262. Hum Reprod. 2018. PMID: 30085138 Clinical Trial.
-
Preimplantation genetic testing for aneuploidies (abnormal number of chromosomes) in in vitro fertilisation.Cochrane Database Syst Rev. 2020 Sep 8;9(9):CD005291. doi: 10.1002/14651858.CD005291.pub3. Cochrane Database Syst Rev. 2020. PMID: 32898291 Free PMC article.
-
Outcomes after assisted reproductive technology in women with cancer: a systematic review and meta-analysis.Hum Reprod. 2023 Jan 5;38(1):30-45. doi: 10.1093/humrep/deac235. Hum Reprod. 2023. PMID: 36342891 Free PMC article.
Cited by
-
Epidemiological characteristics of infertility, 1990-2021, and 15-year forecasts: an analysis based on the global burden of disease study 2021.Reprod Health. 2025 Feb 19;22(1):26. doi: 10.1186/s12978-025-01966-7. Reprod Health. 2025. PMID: 39972325 Free PMC article.
-
Moving toward Narrowing the United States Gap in Assisted Reproductive Technology (ART) Racial and Ethnic Disparities in the Next Decade.J Clin Med. 2024 Apr 11;13(8):2224. doi: 10.3390/jcm13082224. J Clin Med. 2024. PMID: 38673497 Free PMC article. Review.
-
Short and long duration testosterone treatments induce reversable subfertility in female mice using a gestational model of gender-affirming hormone therapy.Hum Reprod. 2025 Apr 1;40(4):695-706. doi: 10.1093/humrep/deaf016. Hum Reprod. 2025. PMID: 39935255
References
-
- Abdulrahim B, Scotland G, Bhattacharya S, Maheshwari A.. Assessing couples’ preferences for fresh or frozen embryo transfer: a discrete choice experiment. Hum Reprod 2021;36:2891–2903. - PubMed
-
- American Society for Reproductive Medicine. Intracytoplasmic sperm injection (ICSI) for non-male factor indications: a committee opinion. Fertil Steril 2020;114:239–245. - PubMed
-
- Barrenetxea G, Garcia-Velasco JA, Aragon B, Osset J, Brosa M, Lopez-Martinez N, Coroleu B.. Comparative economic study of the use of corifollitropin alfa and daily rFSH for controlled ovarian stimulation in older patients: cost-minimization analysis based on the PURSUE study. Reprod Biomed Soc Online 2018;5:46–59. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
