

Obstetric and neonatal outcomes in pregnant women with idiopathic polyhydramnios: a systematic review and meta-analysis
- PMID: 38438422
- PMCID: PMC10912321
- DOI: 10.1038/s41598-024-54840-0
Obstetric and neonatal outcomes in pregnant women with idiopathic polyhydramnios: a systematic review and meta-analysis
Abstract
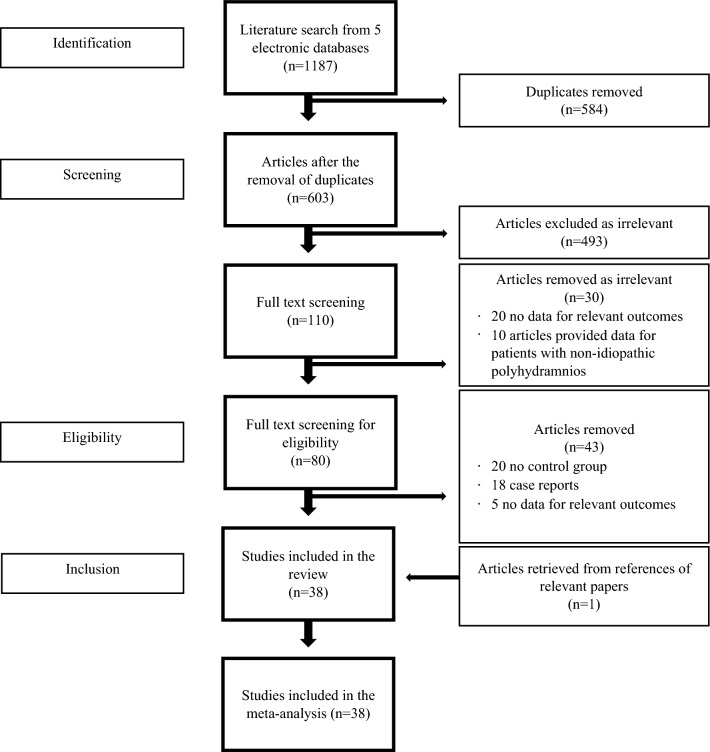
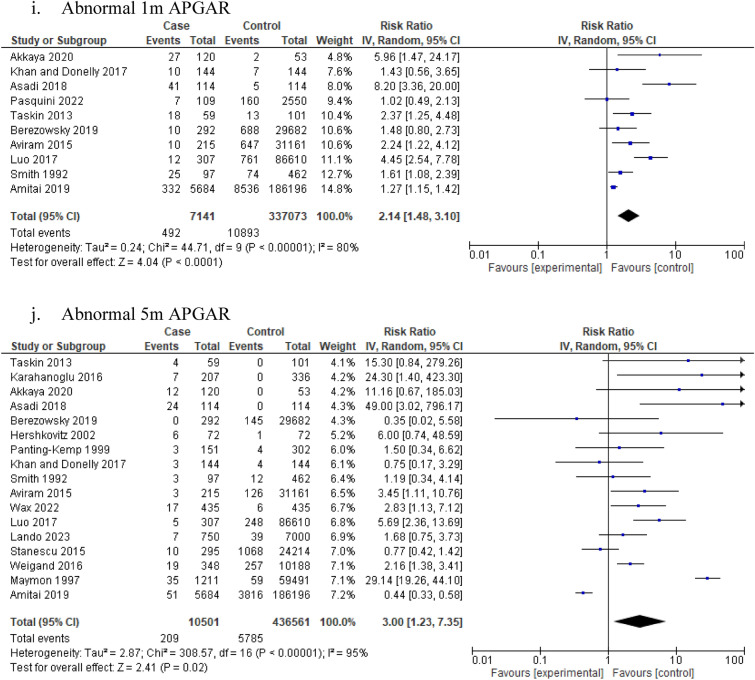
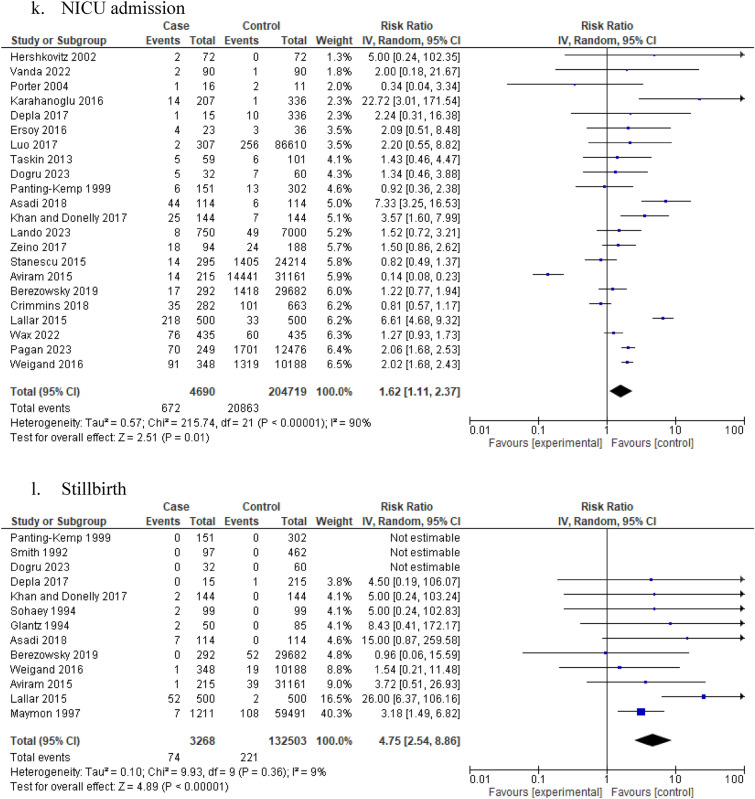
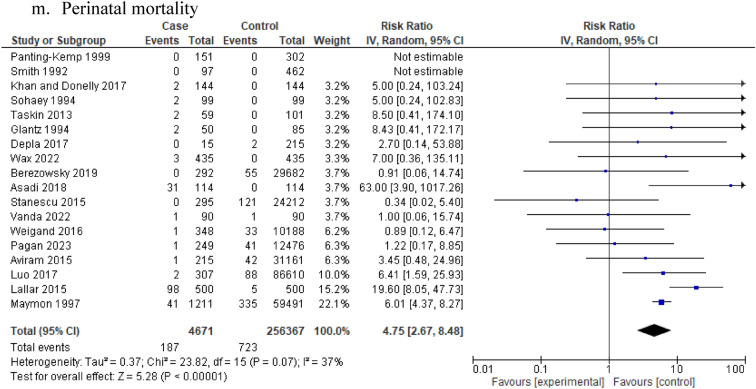
Although the assessment of the amniotic fluid volume in pregnancy is part of the fetal wellbeing surveillance, the impact of idiopathic polyhydramnios (IP) on maternal and perinatal outcomes in unknown. The aim of this meta-analysis was to investigate the association of IP with different maternal and perinatal outcomes. We screened five electronic databases until December 2023 and performed data extraction and quality assessment using ROBINS-E in duplicates. Pooled risk ratios and 95% confidence intervals (95% CI) were calculated with a random effects model. 38 studies were included. Patients with IP were at increased risk of perinatal complications including preterm delivery (RR 1.96, 95% CI 1.35-2.86; I2 = 92%), placental abruption (RR 3.20, 95% CI 2.20-4.65; I2 = 2%), delivery via caesarean section (RR 1.60, 95% CI 1.39-1.84; I2 = 95%) and postpartum haemorrhage (RR 1.98, 95% CI 1.22-3.22; I2 = 84%). Similarly, IP was associated with increased risk of adverse perinatal outcomes including low APGAR score (RR 3.0, 95% CI 1.23-7.35; I2 = 95%), stillbirth (RR 4.75, 95% CI 2.54-8.86; I2 = 9%) and perinatal mortality (RR 4.75, 95% CI 2.67-8.48; I2 = 37%). This meta-analysis suggests that pregnant women with IP may be at increased risk of perinatal complications and adverse neonatal outcomes. However, data remains inconclusive considering the low quality and high heterogeneity of included studies.PROSPERO registration number: CRD42022359944.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Term breech presentation-Intended cesarean section versus intended vaginal delivery-A systematic review and meta-analysis.Acta Obstet Gynecol Scand. 2022 Jun;101(6):564-576. doi: 10.1111/aogs.14333. Acta Obstet Gynecol Scand. 2022. PMID: 35633052 Free PMC article.
-
Impact of preimplantation genetic testing on obstetric and neonatal outcomes: a systematic review and meta-analysis.Fertil Steril. 2021 Oct;116(4):990-1000. doi: 10.1016/j.fertnstert.2021.06.040. Epub 2021 Aug 7. Fertil Steril. 2021. PMID: 34373103
-
Idiopathic Polyhydramnios: Severity and Perinatal Morbidity.Am J Perinatol. 2016 Jun;33(7):658-64. doi: 10.1055/s-0036-1571320. Epub 2016 Feb 10. Am J Perinatol. 2016. PMID: 26862725
-
Transient Idiopathic Polyhydramnios: Maternal and Perinatal Outcomes: Maternal and Perinatal Outcomes.J Ultrasound Med. 2022 Nov;41(11):2859-2866. doi: 10.1002/jum.15974. Epub 2022 Mar 21. J Ultrasound Med. 2022. PMID: 35312096
-
Induction of labour at or beyond 37 weeks' gestation.Cochrane Database Syst Rev. 2020 Jul 15;7(7):CD004945. doi: 10.1002/14651858.CD004945.pub5. Cochrane Database Syst Rev. 2020. PMID: 32666584 Free PMC article.
Cited by
-
Too Much of a Good Thing: Updated Current Management and Perinatal Outcomes of Polyhydramnios.J Med Ultrasound. 2024 Nov 30;32(4):285-290. doi: 10.4103/jmu.jmu_83_24. eCollection 2024 Oct-Dec. J Med Ultrasound. 2024. PMID: 39801544 Free PMC article. Review.
-
Polyhydramnios at Term in Gestational Diabetes: Should We Be Concerned?Children (Basel). 2025 Jul 11;12(7):920. doi: 10.3390/children12070920. Children (Basel). 2025. PMID: 40723113 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
