

Seroprevalence of neuronal antibodies in diseases mimicking autoimmune encephalitis
- PMID: 38438516
- PMCID: PMC10912693
- DOI: 10.1038/s41598-024-55995-6
Seroprevalence of neuronal antibodies in diseases mimicking autoimmune encephalitis
Abstract
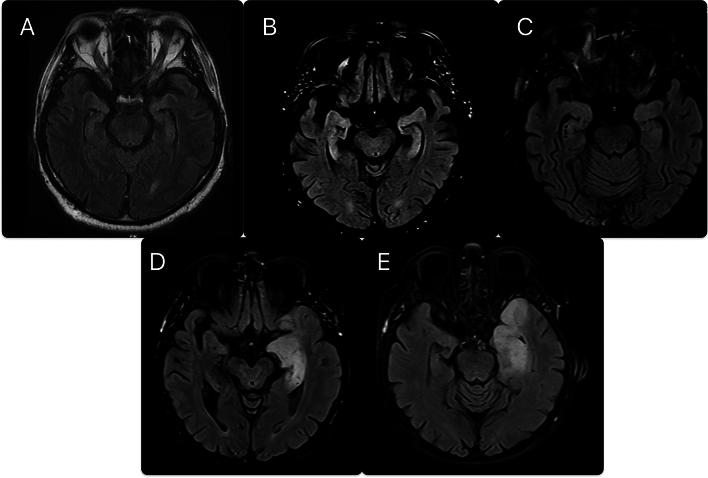
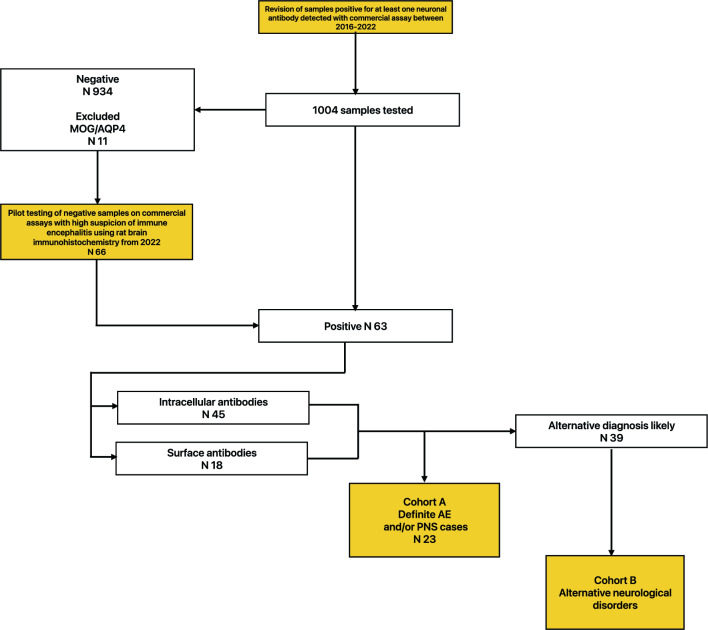
Detection of neuronal antibodies for autoimmune encephalitis and paraneoplastic neurological syndromes relies on commercially available cell-based assays and lineblots. However, lineblots may reveal the presence of neuronal antibodies in patients with various non-autoimmune etiologies. Herein we describe patients with non-autoimmune etiologies (cohort B) and detectable neuronal antibodies and compare them to definite cases of autoimmune encephalitis (cohort A) for differences in clinical data. All patients positive for at least one neuronal antibody were retrospectively evaluated for autoimmune encephalitis and/or paraneoplastic neurological syndrome between 2016 and 2022. 39 cases in cohort B and 23 in cohort A were identified. In cohort B, most common diagnoses were neurodegenerative disorders in 9/39 (23.1%), brain tumors in 6/39 (15.4%) while most common detected antibodies were anti-titin (N10), anti-recoverin (N11), anti-Yo (N8) and all were detected in serum only. Differential aspects between cohort A and B were CSF pleocytosis (14/23 (60.8%) vs 11/35 (31.4%), p = 0.042, respectively), MRI features suggestive of encephalitis (6/23 (26.1%) vs 0 (0%), p = 0.002, respectively) and epilepsy restricted to temporal lobes (14/23 (60.9%) vs 2/30 (6.7%), p = 0.0003, respectively). A large proportion of lineblot results were non-specific when only serum was tested and were frequently found in non-autoimmune neurological conditions.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Autonomic nervous system involvement in autoimmune encephalitis and paraneoplastic neurological syndromes.Rev Neurol (Paris). 2024 Jan-Feb;180(1-2):107-116. doi: 10.1016/j.neurol.2023.12.001. Epub 2023 Dec 22. Rev Neurol (Paris). 2024. PMID: 38142198 Review.
-
Autoimmune encephalitis and paraneoplastic syndromes in Turkey: a multi-centre study.Neurol Sci. 2022 Jul;43(7):4393-4403. doi: 10.1007/s10072-022-05955-7. Epub 2022 Feb 24. Neurol Sci. 2022. PMID: 35211811
-
General features, pathogenesis, and laboratory diagnostics of autoimmune encephalitis.Crit Rev Clin Lab Sci. 2024 Jan;61(1):45-69. doi: 10.1080/10408363.2023.2247482. Epub 2024 Jan 5. Crit Rev Clin Lab Sci. 2024. PMID: 37777038 Review.
-
[Clinical characteristics and short-term outcomes of autoimmune encephalitis in adults].Zh Nevrol Psikhiatr Im S S Korsakova. 2023;123(7. Vyp. 2):103-115. doi: 10.17116/jnevro2023123072103. Zh Nevrol Psikhiatr Im S S Korsakova. 2023. PMID: 37560842 Russian.
-
Glutamate receptor antibodies in neurological diseases: anti-AMPA-GluR3 antibodies, anti-NMDA-NR1 antibodies, anti-NMDA-NR2A/B antibodies, anti-mGluR1 antibodies or anti-mGluR5 antibodies are present in subpopulations of patients with either: epilepsy, encephalitis, cerebellar ataxia, systemic lupus erythematosus (SLE) and neuropsychiatric SLE, Sjogren's syndrome, schizophrenia, mania or stroke. These autoimmune anti-glutamate receptor antibodies can bind neurons in few brain regions, activate glutamate receptors, decrease glutamate receptor's expression, impair glutamate-induced signaling and function, activate blood brain barrier endothelial cells, kill neurons, damage the brain, induce behavioral/psychiatric/cognitive abnormalities and ataxia in animal models, and can be removed or silenced in some patients by immunotherapy.J Neural Transm (Vienna). 2014 Aug;121(8):1029-75. doi: 10.1007/s00702-014-1193-3. Epub 2014 Aug 1. J Neural Transm (Vienna). 2014. PMID: 25081016 Review.
Cited by
-
Anti-recoverin Antibody-Associated Post-acute COVID Vaccination Syndrome After BNT162b2 in HLA-B27-Positive Spondylarthritis: A Case Report.Cureus. 2024 Aug 14;16(8):e66881. doi: 10.7759/cureus.66881. eCollection 2024 Aug. Cureus. 2024. PMID: 39280509 Free PMC article.
References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
