

Topical application of calcitonin gene-related peptide as a regenerative, antifibrotic, and immunomodulatory therapy for corneal injury
- PMID: 38438549
- PMCID: PMC10912681
- DOI: 10.1038/s42003-024-05934-y
Topical application of calcitonin gene-related peptide as a regenerative, antifibrotic, and immunomodulatory therapy for corneal injury
Abstract
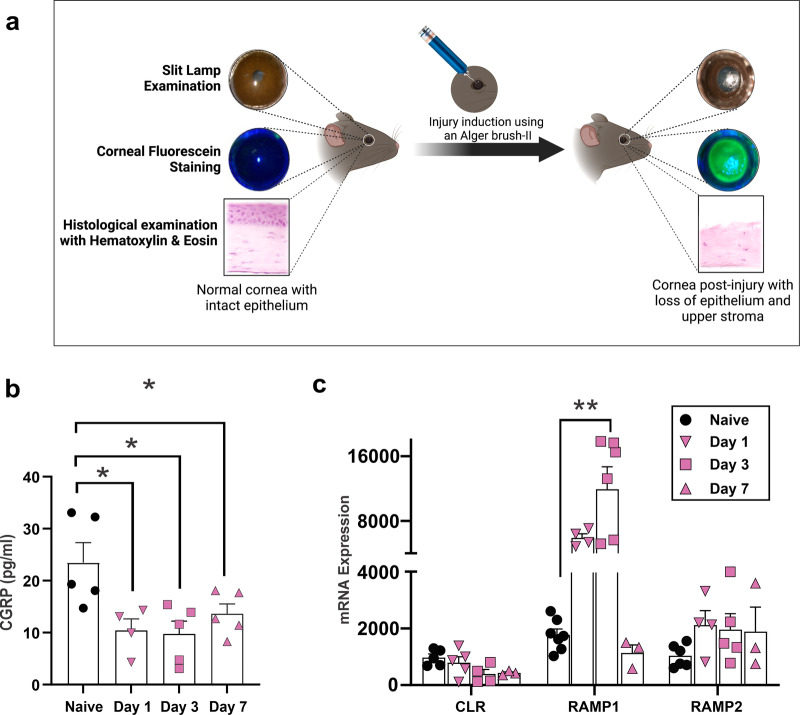
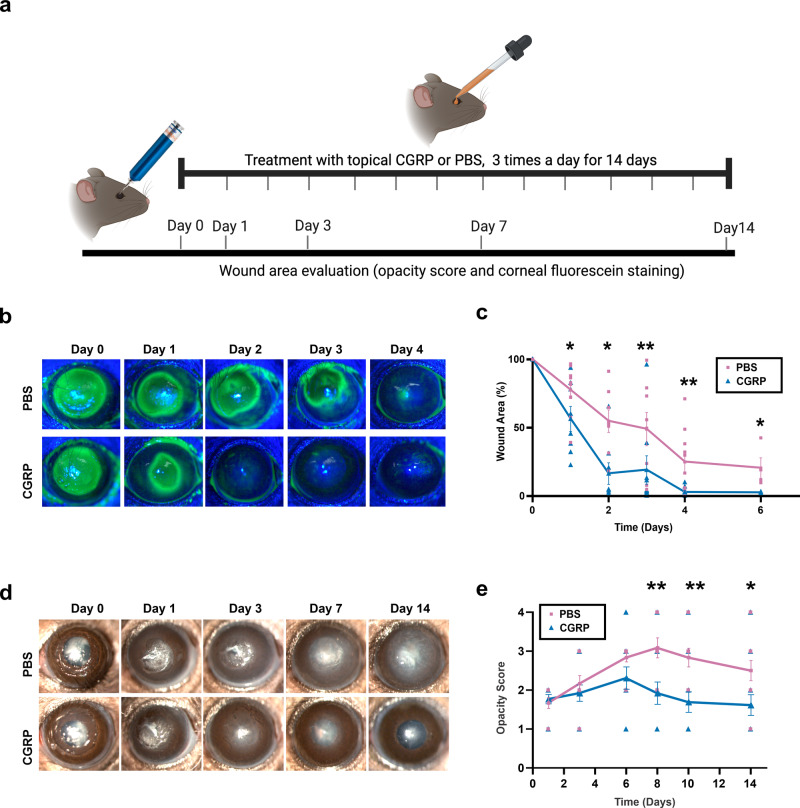
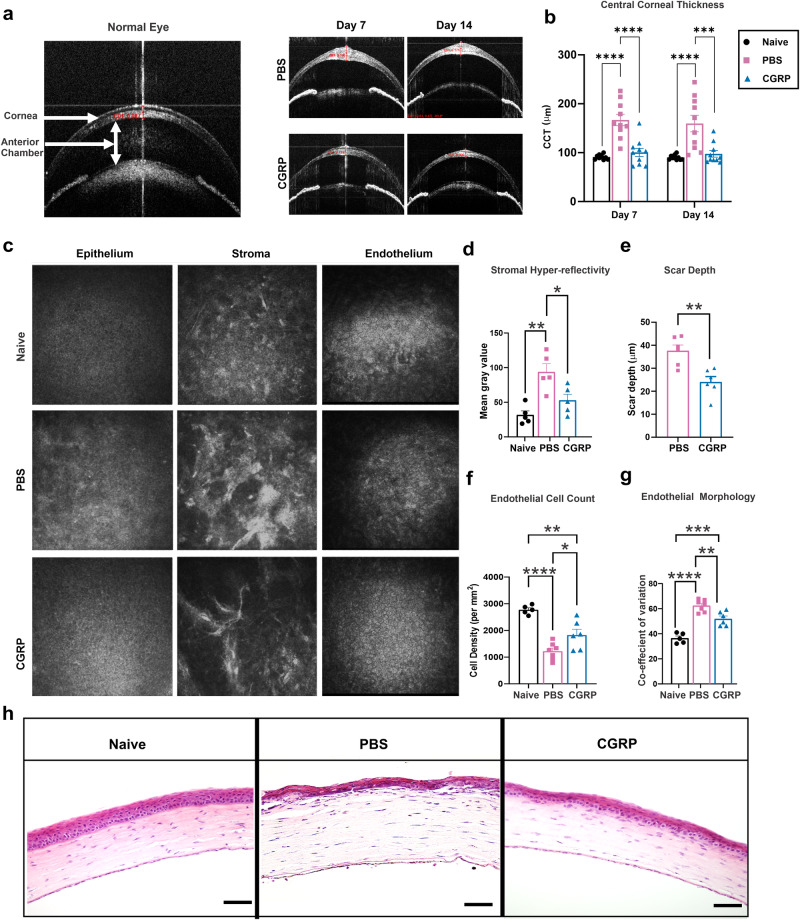
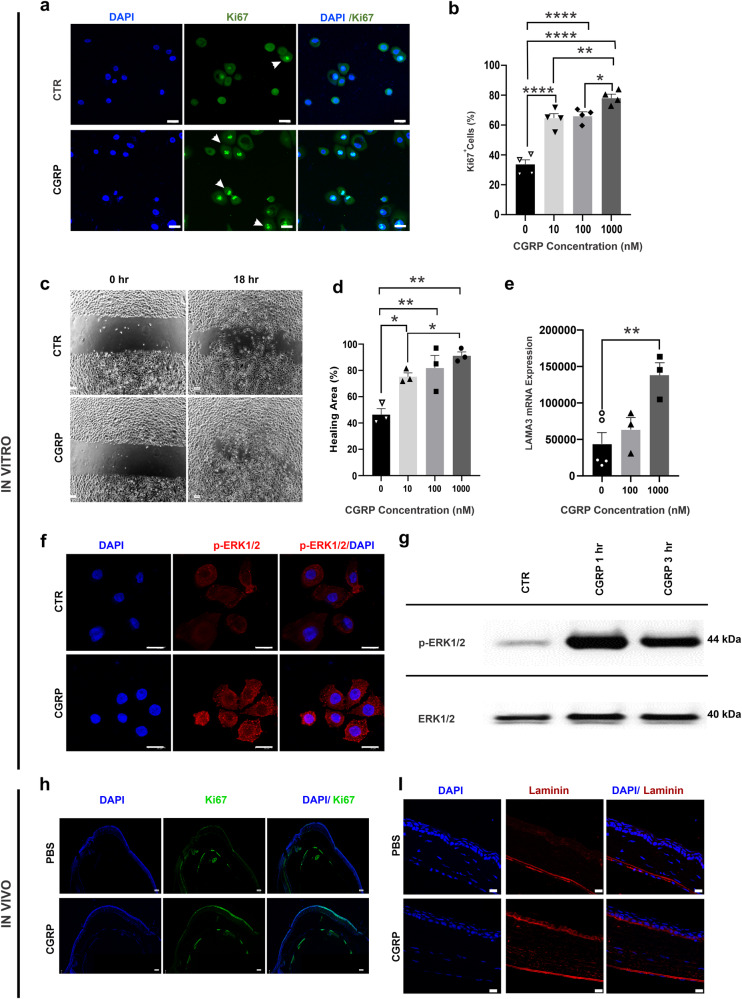
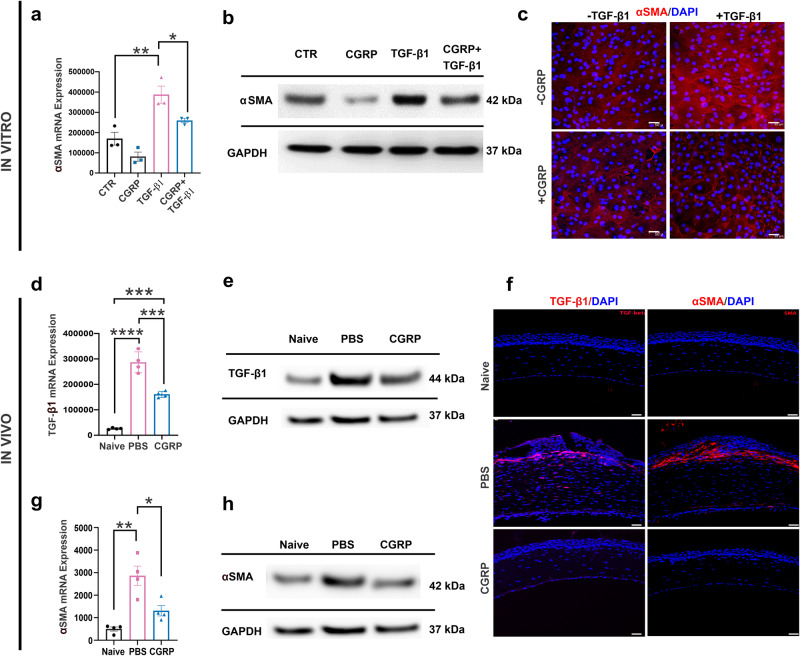
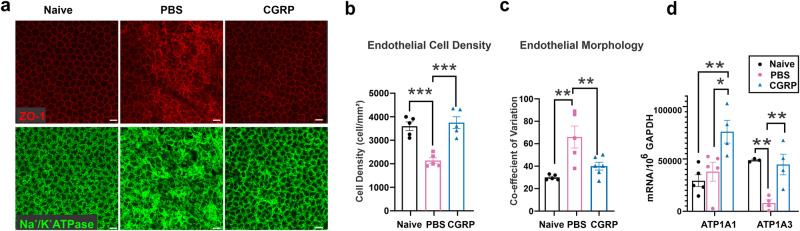
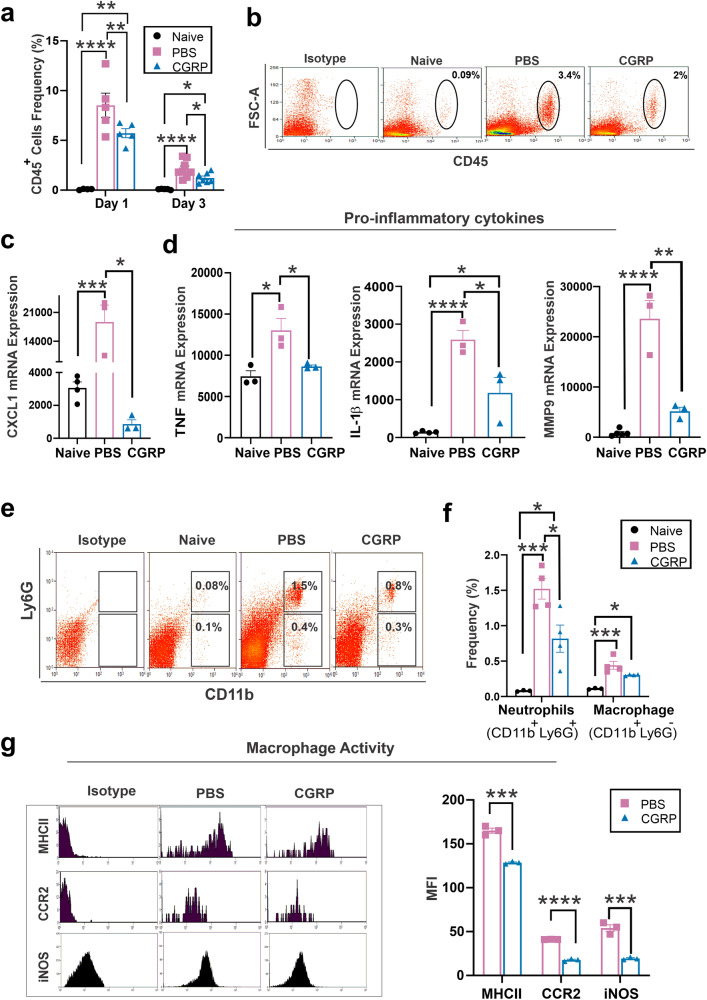
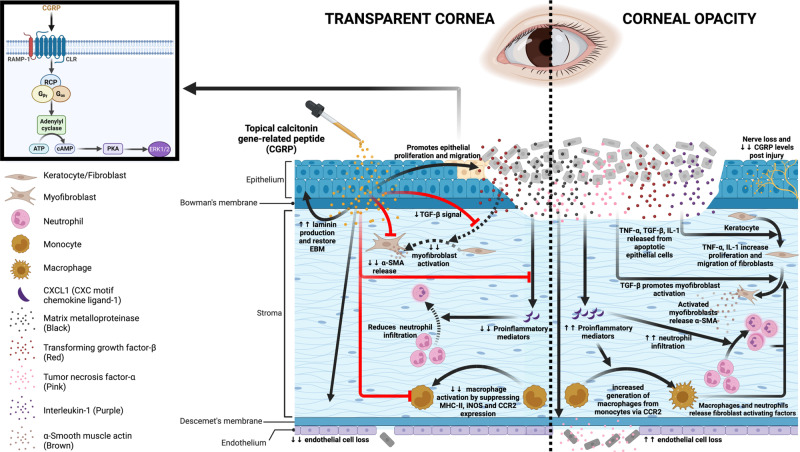
Calcitonin gene-related peptide (CGRP) is a multifunctional neuropeptide abundantly expressed by corneal nerves. Using a murine model of corneal mechanical injury, we found CGRP levels in the cornea significantly reduced after injury. Topical application of CGRP as an eye drop accelerates corneal epithelial wound closure, reduces corneal opacification, and prevents corneal edema after injury in vivo. CGRP promotes corneal epithelial cell migration, proliferation, and the secretion of laminin. It reduces TGF-β1 signaling and prevents TGF-β1-mediated stromal fibroblast activation and tissue fibrosis. CGRP preserves corneal endothelial cell density, morphology, and pump function, thus reducing corneal edema. Lastly, CGRP reduces neutrophil infiltration, macrophage maturation, and the production of inflammatory cytokines in the cornea. Taken together, our results show that corneal nerve-derived CGRP plays a cytoprotective, pro-regenerative, anti-fibrotic, and anti-inflammatory role in corneal wound healing. In addition, our results highlight the critical role of sensory nerves in ocular surface homeostasis and injury repair.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Topical application of calcitonin gene-related peptide as a regenerative, antifibrotic, and immunomodulatory therapy for corneal injury.Res Sq [Preprint]. 2023 Aug 7:rs.3.rs-3204385. doi: 10.21203/rs.3.rs-3204385/v1. Res Sq. 2023. Update in: Commun Biol. 2024 Mar 4;7(1):264. doi: 10.1038/s42003-024-05934-y. PMID: 37609298 Free PMC article. Updated. Preprint.
Similar articles
-
Topical application of calcitonin gene-related peptide as a regenerative, antifibrotic, and immunomodulatory therapy for corneal injury.Res Sq [Preprint]. 2023 Aug 7:rs.3.rs-3204385. doi: 10.21203/rs.3.rs-3204385/v1. Res Sq. 2023. Update in: Commun Biol. 2024 Mar 4;7(1):264. doi: 10.1038/s42003-024-05934-y. PMID: 37609298 Free PMC article. Updated. Preprint.
-
Insulin eye drops improve corneal wound healing in STZ-induced diabetic mice by regulating corneal inflammation and neuropeptide release.BMC Ophthalmol. 2024 Apr 9;24(1):155. doi: 10.1186/s12886-024-03436-3. BMC Ophthalmol. 2024. PMID: 38594682 Free PMC article.
-
The effect of topical decorin on temporal changes to corneal immune cells after epithelial abrasion.J Neuroinflammation. 2022 Apr 12;19(1):90. doi: 10.1186/s12974-022-02444-8. J Neuroinflammation. 2022. PMID: 35414012 Free PMC article.
-
Role of aquaporins in corneal healing post chemical injury.Exp Eye Res. 2023 Mar;228:109390. doi: 10.1016/j.exer.2023.109390. Epub 2023 Jan 22. Exp Eye Res. 2023. PMID: 36696947 Free PMC article. Review.
-
The corneal fibrosis response to epithelial-stromal injury.Exp Eye Res. 2016 Jan;142:110-8. doi: 10.1016/j.exer.2014.09.012. Exp Eye Res. 2016. PMID: 26675407 Free PMC article. Review.
Cited by
-
Tear deficiency transforms spatial distribution of corneal calcitonin gene-related peptide-positive nerves in rats.Front Cell Neurosci. 2025 Jul 1;19:1619310. doi: 10.3389/fncel.2025.1619310. eCollection 2025. Front Cell Neurosci. 2025. PMID: 40666279 Free PMC article.
-
CGRP Released by Corneal Sensory Nerve Maintains Tear Secretion of the Lacrimal Gland.Invest Ophthalmol Vis Sci. 2024 Apr 1;65(4):30. doi: 10.1167/iovs.65.4.30. Invest Ophthalmol Vis Sci. 2024. PMID: 38635244 Free PMC article.
-
CGRP sensory neurons promote tissue healing via neutrophils and macrophages.Nature. 2024 Apr;628(8008):604-611. doi: 10.1038/s41586-024-07237-y. Epub 2024 Mar 27. Nature. 2024. PMID: 38538784 Free PMC article.
-
Calcitonin Gene-Related Peptide Regulates Specific Interferon-Stimulating Genes to Inhibit Apoptosis of Corneal Epithelial Cells in Dry Eye Disease.Invest Ophthalmol Vis Sci. 2025 Jul 1;66(9):65. doi: 10.1167/iovs.66.9.65. Invest Ophthalmol Vis Sci. 2025. PMID: 40728362 Free PMC article.
-
The healing power of sensory neurons: New horizons for diabetic and neuropathic tissue repair.Clin Transl Med. 2024 Aug;14(8):e1813. doi: 10.1002/ctm2.1813. Clin Transl Med. 2024. PMID: 39166883 Free PMC article. No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
