

CAR T therapies in multiple myeloma: unleashing the future
- PMID: 38438559
- PMCID: PMC11101341
- DOI: 10.1038/s41417-024-00750-2
CAR T therapies in multiple myeloma: unleashing the future
Abstract
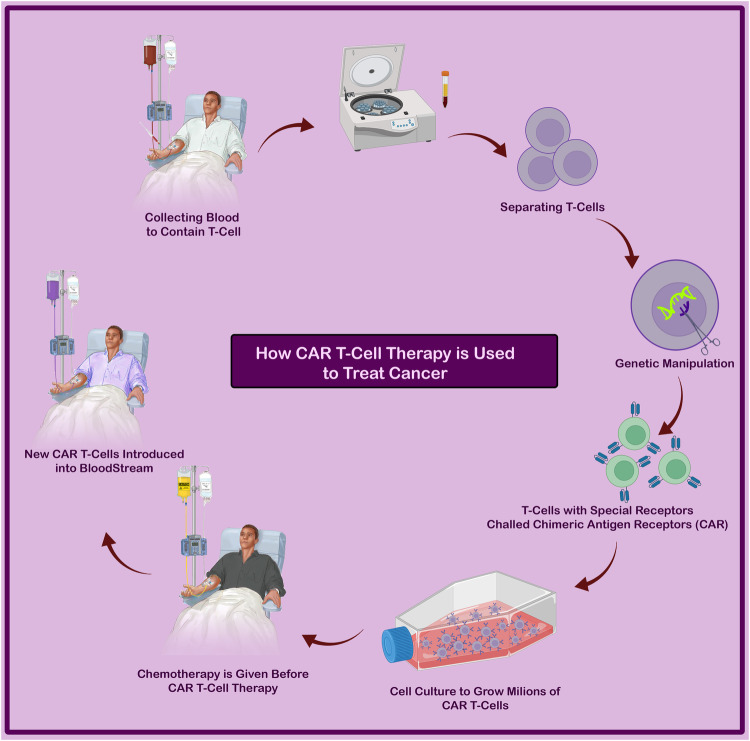
In recent years, the field of cancer treatment has witnessed remarkable breakthroughs that have revolutionized the landscape of care for cancer patients. While traditional pillars such as surgery, chemotherapy, and radiation therapy have long been available, a cutting-edge therapeutic approach called CAR T-cell therapy has emerged as a game-changer in treating multiple myeloma (MM). This novel treatment method complements options like autologous stem cell transplants and immunomodulatory medications, such as proteasome inhibitors, by utilizing protein complexes or anti-CD38 antibodies with potent complement-dependent cytotoxic effects. Despite the challenges and obstacles associated with these treatments, the recent approval of the second FDA multiple myeloma CAR T-cell therapy has sparked immense promise in the field. Thus far, the results indicate its potential as a highly effective therapeutic solution. Moreover, ongoing preclinical and clinical trials are exploring the capabilities of CAR T-cells in targeting specific antigens on myeloma cells, offering hope for patients with relapsed/refractory MM (RRMM). These advancements have shown the potential for CAR T cell-based medicines or combination therapies to elicit greater treatment responses and minimize side effects. In this context, it is crucial to delve into the history and functions of CAR T-cells while acknowledging their limitations. We can strategize and develop innovative approaches to overcome these barriers by understanding their challenges. This article aims to provide insights into the application of CAR T-cells in treating MM, shedding light on their potential, limitations, and strategies employed to enhance their efficacy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Cancer Stat Facts: Myeloma. https://seer.cancer.gov/seertools/hemelymph/ (2022).
-
- Kazmi SM, Nusrat M, Gunaydin H, Cornelison AM, Shah N, Kebriaei P, et al. Outcomes among high-risk and standard-risk multiple myeloma patients treated with high-dose chemotherapy and autologous hematopoietic stem-cell transplantation. Clin Lymphoma Myeloma Leuk. 2015;15:687–93. doi: 10.1016/j.clml.2015.07.641. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
