

Prognosis of LSPD versus TIPS for the treatment of esophagogastric variceal bleeding in cirrhosis
- PMID: 38438672
- PMCID: PMC10978701
- DOI: 10.1007/s00464-024-10729-7
Prognosis of LSPD versus TIPS for the treatment of esophagogastric variceal bleeding in cirrhosis
Abstract
Background: This study aimed to compare postoperative complications in patients with esophagogastric variceal bleeding (EVB) who underwent laparoscopic splenectomy combined with pericardial devascularization (LSPD) versus transjugular intrahepatic portosystemic shunt (TIPS) procedures.
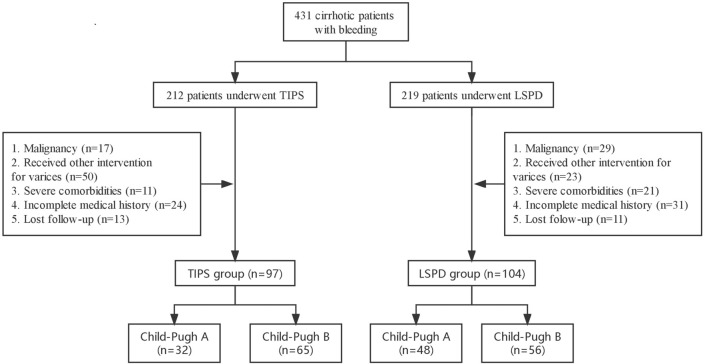
Methods: A retrospective collection of medical records was conducted from January 2014 to May 2020 at Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. The study included patients from the departments of trauma surgery, interventional radiology, and general surgery who were diagnosed with EVB caused by portal hypertension and treated with LSPD or TIPS. Follow-up data were obtained to assess the occurrence of postoperative complications in both groups.
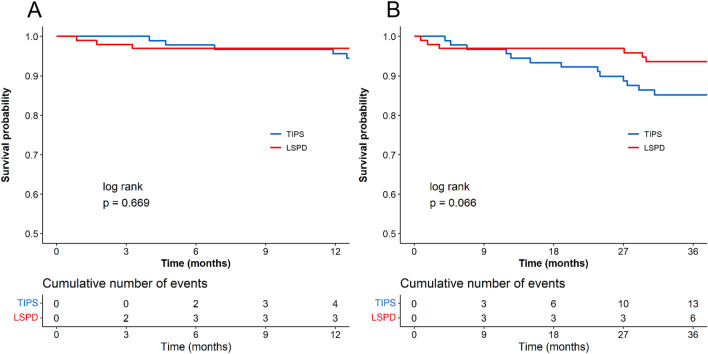
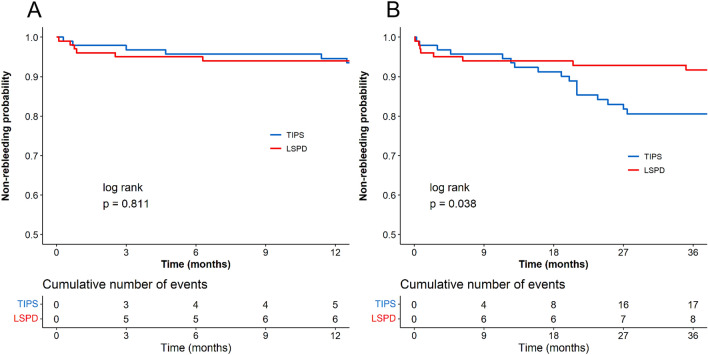
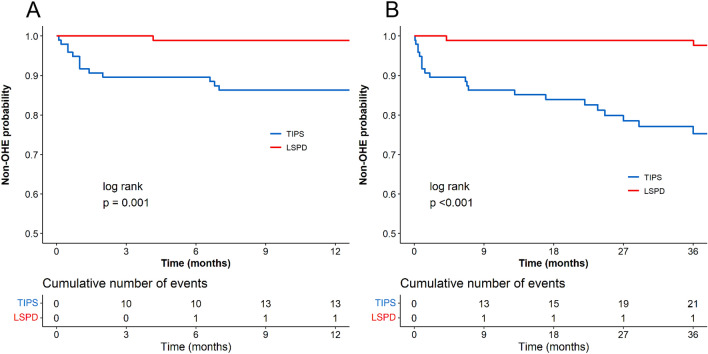
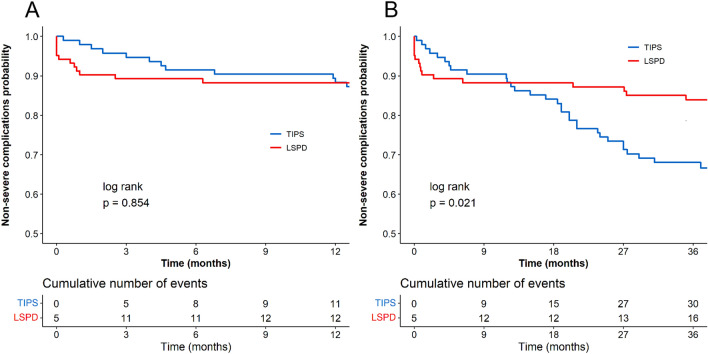
Results: A total of 201 patients were included in the study, with 104 cases in the LSPD group and 97 cases in the TIPS group. There was no significant difference in the 1-year and 3-year post-surgery survival rates between the TIPS and LSPD groups (P = 0.669, 0.066). The 3-year survival rate of Child-Pugh B patients in the LSPD group was higher than TIPS group (P = 0.041). The LSPD group also had a significantly higher rate of freedom from rebleeding at 3-year post-surgery compared to the TIPS group (P = 0.038). Stratified analysis showed no statistically significant difference in the rebleeding rate between the two groups. Furthermore, the LSPD group had a higher rate of freedom from overt hepatic encephalopathy at 1-year and 3-year post-surgery compared to the TIPS group (P = 0.007, < 0.001). The LSPD group also had a lower rate of severe complications at 3-year post-surgery compared to the TIPS group (P = 0.020).
Conclusion: Compared to TIPS, LSPD does not increase the risk of mortality and rebleeding, while demonstrating fewer complications. In patients classified as Child-Pugh A and B, the use of LSPD for treating EVB is both safe and effective.
Keywords: Esophagogastric variceal bleeding; Laparoscopic splenectomy combined with pericardial devascularization; Portal hypertension; Transjugular intrahepatic portosystemic shunt.
© 2024. The Author(s).
Conflict of interest statement
Biao Chen, Jingxuan Wang, Weiyong Sheng, Bingqing Ma, Peng Xu, Xing Cheng, Weiyi Cheng, Chengjun Cai, Guoliang Wang, Wenming Pan, Chidan Wan, Chuansheng Zheng, Ping Cheng, and Jinxiang Zhang have no conflicts of interest or financial ties to disclose.
Figures
Similar articles
-
Transjugular intrahepatic portosystemic shunt versus open splenectomy and esophagogastric devascularization for portal hypertension with recurrent variceal bleeding.Hepatobiliary Pancreat Dis Int. 2017 Apr;16(2):169-175. doi: 10.1016/s1499-3872(16)60129-7. Hepatobiliary Pancreat Dis Int. 2017. PMID: 28381381
-
Transjugular intrahepatic portosystemic shunt (TIPS) versus laparoscopic splenectomy (LS) plus preoperative endoscopic varices ligation (EVL) in the treatment of recurrent variceal bleeding.Surg Endosc. 2013 Aug;27(8):2712-20. doi: 10.1007/s00464-013-2810-1. Epub 2013 Feb 8. Surg Endosc. 2013. PMID: 23392981
-
Comparison of long-term outcomes of splenectomy with periesophagogastric devascularization and transjugular intrahepatic portosystemic shunt in treating cirrhotic portal hypertension patients with recurrent variceal bleeding.Langenbecks Arch Surg. 2023 May 29;408(1):215. doi: 10.1007/s00423-023-02933-1. Langenbecks Arch Surg. 2023. PMID: 37247018 Free PMC article.
-
Surgical portosystemic shunts versus transjugular intrahepatic portosystemic shunt for variceal haemorrhage in people with cirrhosis.Cochrane Database Syst Rev. 2018 Oct 31;10(10):CD001023. doi: 10.1002/14651858.CD001023.pub3. Cochrane Database Syst Rev. 2018. PMID: 30378107 Free PMC article.
-
The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension.J Clin Gastroenterol. 2007 Nov-Dec;41 Suppl 3:S344-51. doi: 10.1097/MCG.0b013e318157e500. J Clin Gastroenterol. 2007. PMID: 17975487 Review.
Cited by
-
Refractory massive chylothorax following robot-assisted laparoscopic splenectomy with pericardial devascularization treated with trans-jugular intrahepatic portosystemic shunt: a case report.Front Med (Lausanne). 2024 Sep 4;11:1420157. doi: 10.3389/fmed.2024.1420157. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39296890 Free PMC article.
References
-
- Lianyue Y, Xueli B. Expert consensus on diagnosis and treatment of esophagogastric variceal bleeding in cirrhotic portal hypertension (2019 edition) Chinese Journal of Surgery. 2019;57(12):885–892. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
