

Quantitative whole-body muscle MRI in idiopathic inflammatory myopathies including polymyositis with mitochondrial pathology: indications for a disease spectrum
- PMID: 38438820
- PMCID: PMC11136737
- DOI: 10.1007/s00415-024-12191-w
Quantitative whole-body muscle MRI in idiopathic inflammatory myopathies including polymyositis with mitochondrial pathology: indications for a disease spectrum
Abstract
Objective: Inflammatory myopathies (IIM) include dermatomyositis (DM), sporadic inclusion body myositis (sIBM), immune-mediated necrotizing myopathy (IMNM), and overlap myositis (OLM)/antisynthetase syndrome (ASyS). There is also a rare variant termed polymyositis with mitochondrial pathology (PM-Mito), which is considered a sIBM precursor. There is no information regarding muscle MRI for this rare entity. The aim of this study was to compare MRI findings in IIM, including PM-Mito.
Methods: This retrospective analysis included 41 patients (7 PM-Mito, 11 sIBM, 11 PM/ASyS/OLM, 12 IMNM) and 20 healthy controls. Pattern of muscle involvement was assessed by semiquantitative evaluation, while Dixon method was used to quantify muscular fat fraction.
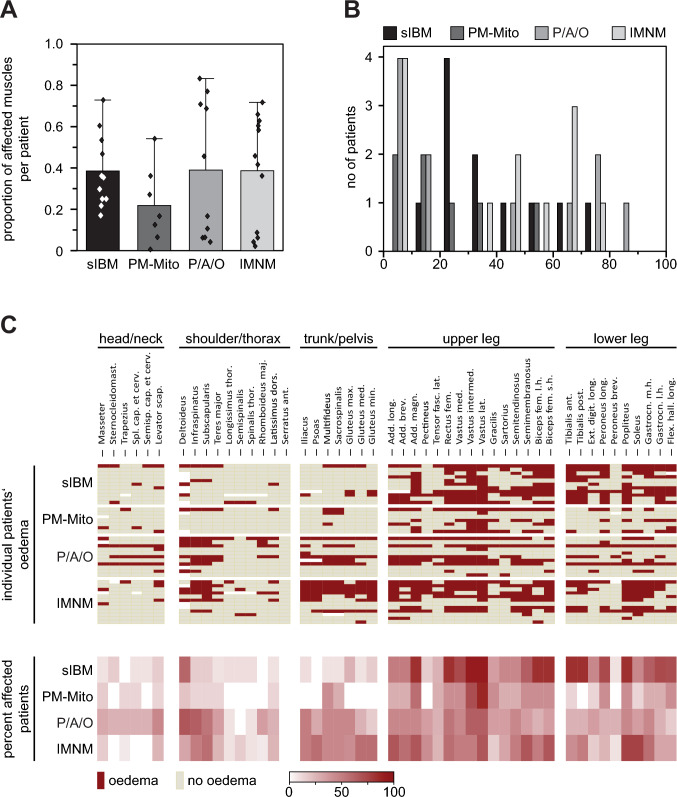
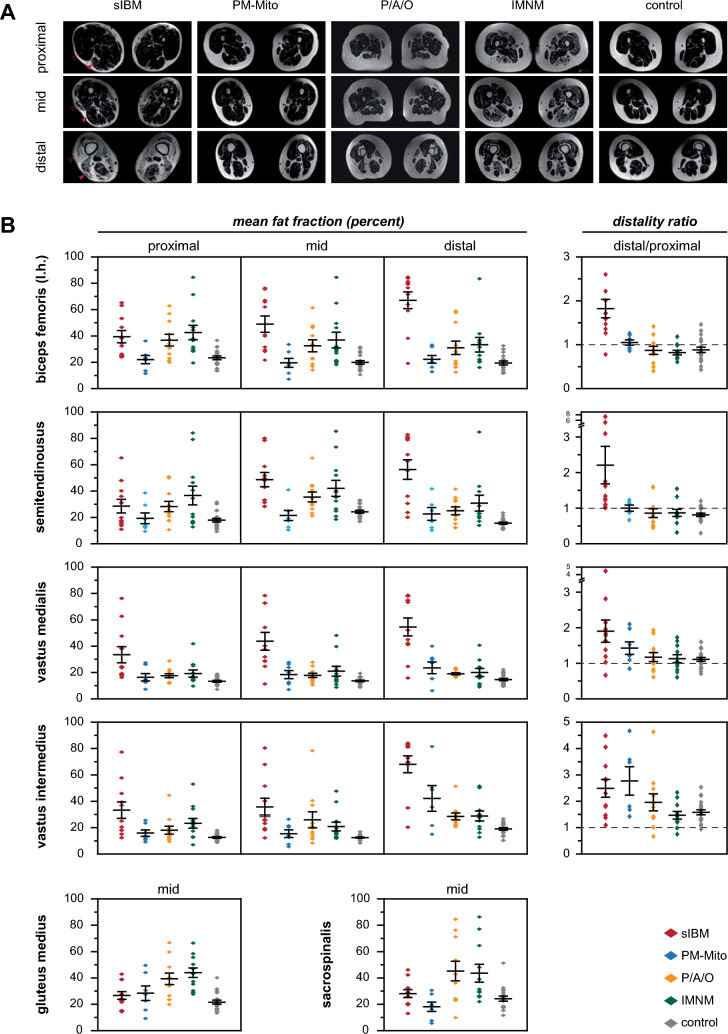
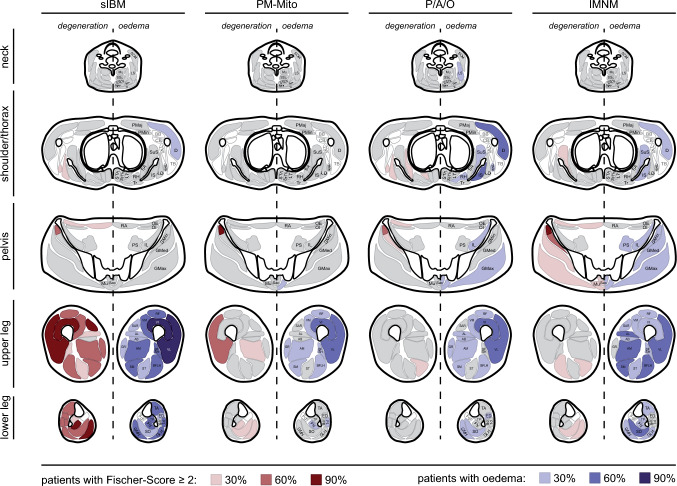
Results: The sIBM typical pattern affecting the lower extremities was not found in the majority of PM-Mito-patients. Intramuscular edema in sIBM and PM-Mito was limited to the lower extremities, whereas IMNM and PM/ASyS/OLM showed additional edema in the trunk. Quantitative assessment showed increased fat content in sIBM, with an intramuscular proximo-distal gradient. Similar changes were also found in a few PM-Mito- and PM/ASyS/OLM patients. In sIBM and PM-Mito, mean fat fraction of several muscles correlated with clinical involvement.
Interpretation: As MRI findings in patients with PM-Mito relevantly differed from sIBM, the attribution of PM-Mito as sIBM precursor should be critically discussed. Some patients in PM/ASyS/OLM and PM-Mito group showed MR-morphologic features predominantly observed in sIBM, indicative of a spectrum from PM/ASyS/OLM toward sIBM. In some IIM subtypes, MRI may serve as a biomarker of disease severity.
Keywords: IBM; Imaging biomarker; Inclusion body myositis; Myositis; PM-Mito; qMRI.
© 2024. The Author(s).
Conflict of interest statement
The authors report no conflicts of interest.
Figures


References
-
- Lundberg IE, Fujimoto M, Vencovsky J, et al. Idiopathic inflammatory myopathies. Nat Rev Dis Primers. 2021;7:86. - PubMed
-
- Uruha A, Goebel H-H, Stenzel W. Updates on the immunopathology in idiopathic inflammatory myopathies. Curr Rheumatol Rep. 2021;23:56. - PubMed
-
- Tanboon J, Uruha A, Stenzel W, Nishino I. Where are we moving in the classification of idiopathic inflammatory myopathies? Curr Opin Neurol. 2020;33:590–603. - PubMed
-
- Ashton C, Paramalingam S, Stevenson B, et al. Idiopathic inflammatory myopathies: a review. Intern Med J. 2021;51:845–852. - PubMed
-
- Benveniste O, Stenzel W, Allenbach Y. Advances in serological diagnostics of inflammatory myopathies. Curr Opin Neurol. 2016;29:662–673. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
