

Effect of Postoperative Prolonged sedation with Dexmedetomidine after successful reperfusion with Endovascular Thrombectomy on long-term prognosis in patients with acute ischemic stroke (PPDET): study protocol for a randomized controlled trial
- PMID: 38439027
- PMCID: PMC10913237
- DOI: 10.1186/s13063-024-08015-x
Effect of Postoperative Prolonged sedation with Dexmedetomidine after successful reperfusion with Endovascular Thrombectomy on long-term prognosis in patients with acute ischemic stroke (PPDET): study protocol for a randomized controlled trial
Abstract
Background: Endovascular thrombectomy (EVT) is a standard treatment for acute ischemic stroke (AIS) with large vessel occlusion. Hypertension and increased blood pressure variability within the first 24 h after successful reperfusion are related to a higher risk of symptomatic intracerebral hemorrhage and higher mortality. AIS patients might suffer from ischemia-reperfusion injury following reperfusion, especially within 24 h. Dexmedetomidine (DEX), a sedative commonly used in EVT, can stabilize hemodynamics by inhibiting the sympathetic nervous system and alleviate ischemia-reperfusion injury through anti-inflammatory and antioxidative properties. Postoperative prolonged sedation for 24 h with DEX might be a potential pharmacological approach to improve long-term prognosis after EVT.
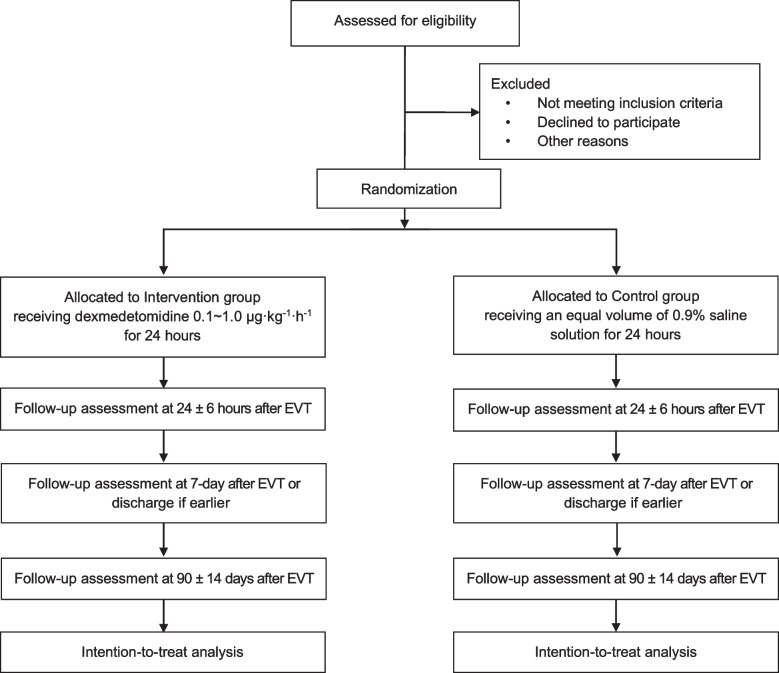
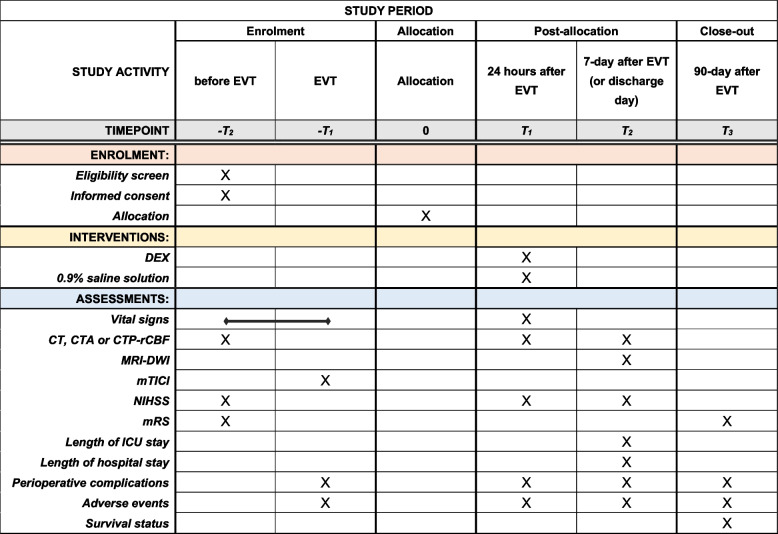
Methods: This single-center, open-label, prospective, randomized controlled trial will include 368 patients. The ethics committee has approved the protocol. After successful reperfusion (modified thrombolysis in cerebral infarction scores 2b-3, indicating reperfusion of at least 50% of the affected vascular territory), participants are randomly assigned to the intervention or control group. In the intervention group, participants will receive 0.1~1.0 μg/kg/h DEX for 24 h. In the control group, participants will receive an equal dose of saline for 24 h. The primary outcome is the functional outcome at 90 days, measured with the categorical scale of the modified Rankin Scale, ranging from 0 (no symptoms) to 6 (death). The secondary outcome includes (1) the changes in stroke severity between admission and 24 h and 7 days after EVT, measured by the National Institute of Health Stroke Scale (ranging from 0 to 42, with higher scores indicating greater severity); (2) the changes in ischemic penumbra volume/infarct volume between admission and 7 days after EVT, measured by neuroimaging scan; (3) the length of ICU/hospital stay; and (4) adverse events and the all-cause mortality rate at 90 days.
Discussion: This randomized clinical trial is expected to verify the hypothesis that postoperative prolonged sedation with DEX after successful reperfusion may promote the long-term prognosis of patients with AIS and may reduce the related socio-economic burden.
Trial registration: ClinicalTrials.gov NCT04916197. Prospectively registered on 7 June 2021.
Keywords: Acute ischemic stroke; Dexmedetomidine; Endovascular thrombectomy; Postoperative prolonged sedation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Feigin VL, Stark BA, Johnson CO, Roth GA, Bisignano C, Abady GG, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi: 10.1016/S1474-4422(21)00252-0. - DOI - PMC - PubMed
-
- Patel P, Yavagal D, Khandelwal P. Hyperacute management of ischemic strokes: JACC Focus Seminar [Internet]. Vol. 75, Journal of the American College of Cardiology. J Am Coll Cardiol; 2020 [cited 2021 Oct 9]. p. 1844–56. Available from: http://www.ncbi.nlm.nih.gov/pubmed/32299596. - PubMed
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study [Internet]. Vol. 76, Journal of the American College of Cardiology. J Am Coll Cardiol; 2020 [cited 2021 Oct 9]. p. 2982–3021. Available from: http://www.ncbi.nlm.nih.gov/pubmed/33309175. - PMC - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke A. Stroke. 2019;50:E344–E418. doi: 10.1161/STR.0000000000000211. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
