

A risk analysis of alpelisib-induced hyperglycemia in patients with advanced solid tumors and breast cancer
- PMID: 38439079
- PMCID: PMC10913434
- DOI: 10.1186/s13058-024-01773-1
A risk analysis of alpelisib-induced hyperglycemia in patients with advanced solid tumors and breast cancer
Abstract
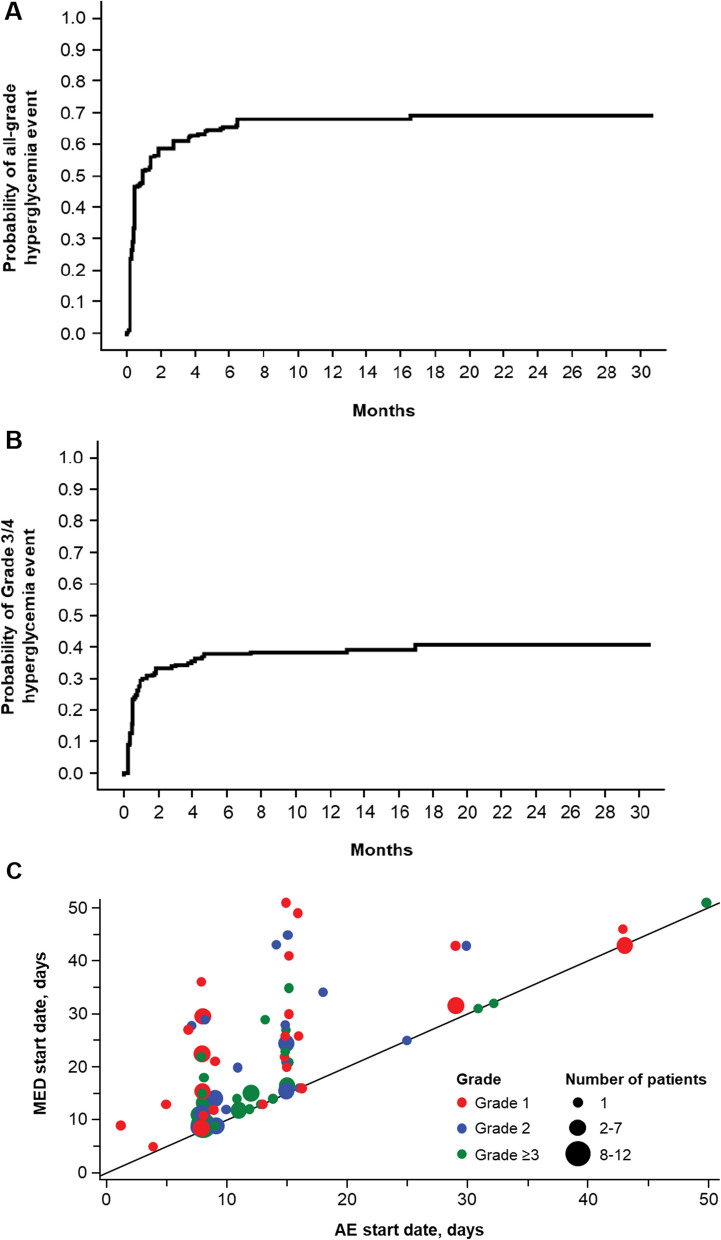
Background: Hyperglycemia is an on-target effect of PI3Kα inhibitors. Early identification and intervention of treatment-induced hyperglycemia is important for improving management of patients receiving a PI3Kα inhibitor like alpelisib. Here, we characterize incidence of grade 3/4 alpelisib-related hyperglycemia, along with time to event, management, and outcomes using a machine learning model.
Methods: Data for the risk model were pooled from patients receiving alpelisib ± fulvestrant in the open-label, phase 1 X2101 trial and the randomized, double-blind, phase 3 SOLAR-1 trial. The pooled population (n = 505) included patients with advanced solid tumors (X2101, n = 221) or HR+/HER2- advanced breast cancer (SOLAR-1, n = 284). External validation was performed using BYLieve trial patient data (n = 340). Hyperglycemia incidence and management were analyzed for SOLAR-1.
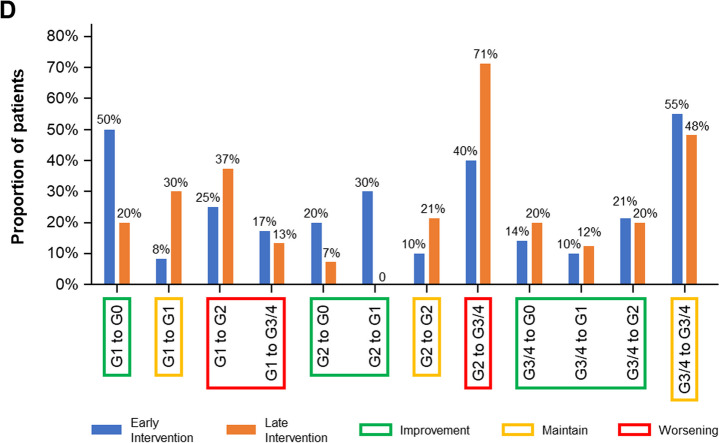
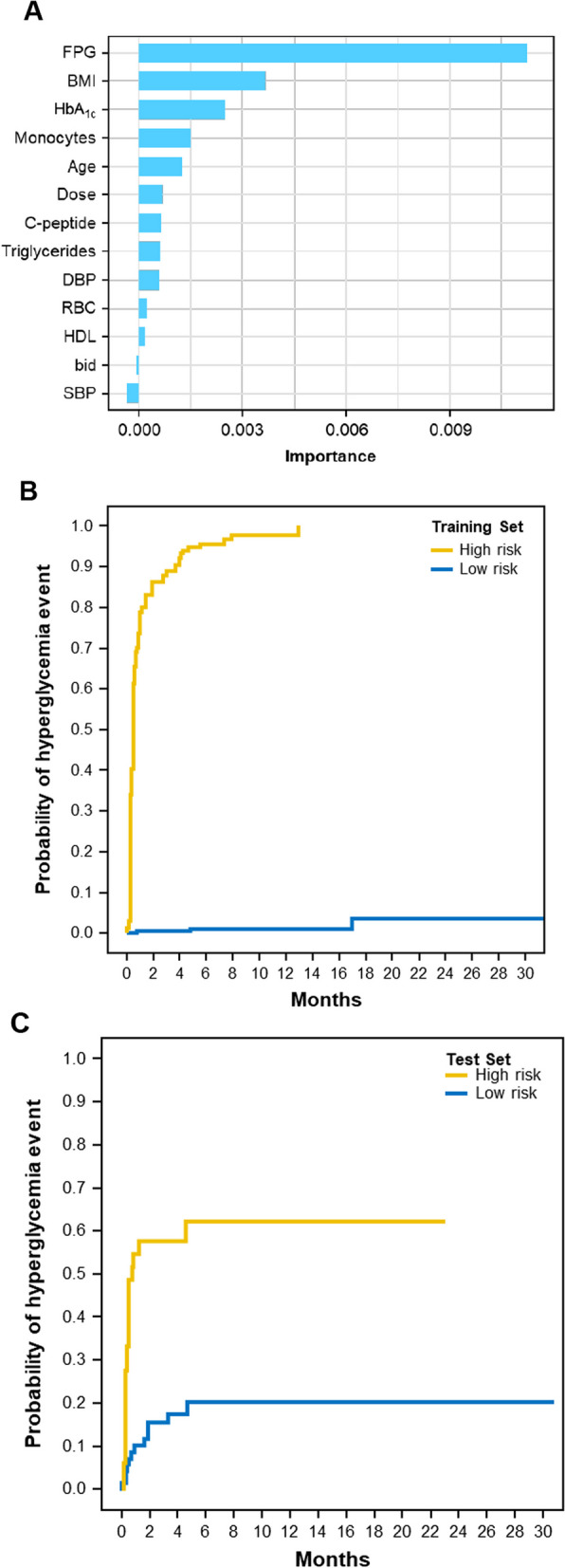
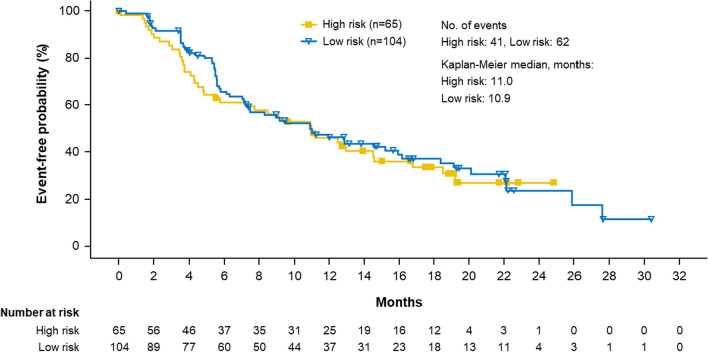
Results: A random forest model identified 5 baseline characteristics most associated with risk of developing grade 3/4 hyperglycemia (fasting plasma glucose, body mass index, HbA1c, monocytes, age). This model was used to derive a score to classify patients as high or low risk for developing grade 3/4 hyperglycemia. Applying the model to patients treated with alpelisib and fulvestrant in SOLAR-1 showed higher incidence of hyperglycemia (all grade and grade 3/4), increased use of antihyperglycemic medications, and more discontinuations due to hyperglycemia (16.7% vs. 2.6% of discontinuations) in the high- versus low-risk group. Among patients in SOLAR-1 (alpelisib + fulvestrant arm) with PIK3CA mutations, median progression-free survival was similar between the high- and low-risk groups (11.0 vs. 10.9 months). For external validation, the model was applied to the BYLieve trial, for which successful classification into high- and low-risk groups with shorter time to grade 3/4 hyperglycemia in the high-risk group was observed.
Conclusions: A risk model using 5 clinically relevant baseline characteristics was able to identify patients at higher or lower probability for developing alpelisib-induced hyperglycemia. Early identification of patients who may be at higher risk for hyperglycemia may improve management (including monitoring and early intervention) and potentially lead to improved outcomes.
Registration: ClinicalTrials.gov: NCT01219699 (registration date: October 13, 2010; retrospectively registered), ClinicalTrials.gov: NCT02437318 (registration date: May 7, 2015); ClinicalTrials.gov: NCT03056755 (registration date: February 17, 2017).
Keywords: Alpelisib; BYLieve; HR+/HER2− advanced breast cancer; Hyperglycemia; Machine learning; SOLAR-1.
© 2024. The Author(s).
Conflict of interest statement
Jordi Rodón reports receiving consulting and travel fees from Novartis, Eli Lilly, Orion Pharmaceuticals, Servier Pharmaceuticals, Peptomyc, Merck Sharp & Dohme, Kelun Pharmaceutical/Klus Pharma, Spectrum Pharmaceuticals Inc, Pfizer, Roche Pharmaceuticals, Ellipses Pharma, NovellusDx, Ionctura and Molecular Partners (including serving on the scientific advisory board from 2015-present), receiving research funding from Blueprint Pharmaceuticals, Bayer and Novartis; David Demanse, Huilin Hu, Dragica Vuina, Cornelia Quadt report employment and stock ownership from Novartis; Hope S. Rugo reports grants from Plexxikon, Macrogenics, OBI Pharma, Eisai, Pfizer, Novartis, Eli Lilly, GlaxoSmithKline, Genentech, Celsion, Merck; fees for travel, accommodations, and expenses from Novartis, Roche/Genentech, OBI Pharma, Bayer, and Pfizer; speaker’s bureau for Genomic Health; Howard A. Burris, Rafael Simó, Melissa F. Wellons have nothing to report; Azeez Farooki reports being a member of a data safety monitoring board for a current Novartis study; Fabrice André reports research funding from AstraZeneca, Lilly, Novartis, Pfizer, Roche; Dejan Juric reports scientific advisory board for Novartis, Genentech, Eisai, Ipsen, EMD Serono.
Figures
References
-
- Mollon L, Aguilar A, Anderson E, Dean J, Davis L, Warholak T, Aizer AA, Platt E, Bardiya A, Tang D. A systematic literature review of the prevalence of PIK3CA mutations and mutation hotspots in HR+/HER2-metastatic breast cancer. Cancer Res. 2018;78(13_Supplement):1207. doi: 10.1158/1538-7445.AM2018-1207. - DOI
-
- National Comprehensive Cancer Network. Breast cancer V4.2023. https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
