

Opioid analgesia and severity of acute pancreatitis: An international multicentre cohort study on pain management in acute pancreatitis
- PMID: 38439202
- PMCID: PMC11017759
- DOI: 10.1002/ueg2.12542
Opioid analgesia and severity of acute pancreatitis: An international multicentre cohort study on pain management in acute pancreatitis
Abstract
Background: The effect of analgesic modalities on short-term outcomes in acute pancreatitis remains unknown. However, preclinical models have raised safety concerns regarding opioid use in patients with acute pancreatitis.
Objective: This study aimed to assess the association between analgesics, particularly opioids, and severity and mortality in hospitalised patients with acute pancreatitis.
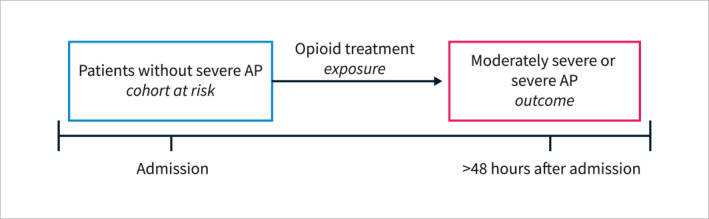
Methods: This prospective multicentre cohort study recruited consecutive patients admitted with a first episode of acute pancreatitis between April 1 and 30 June 2022, with a 1-month follow-up. Data on aetiology, clinical course, and analgesic treatment were collected. The primary outcome was the association between opioid analgesia and acute pancreatitis severity, which was analysed using univariate and multivariate analyses.
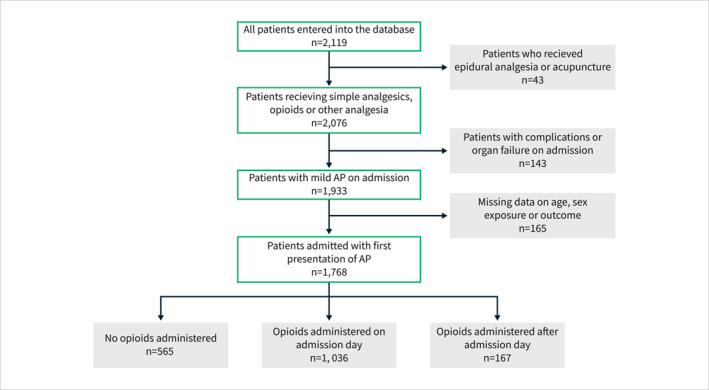
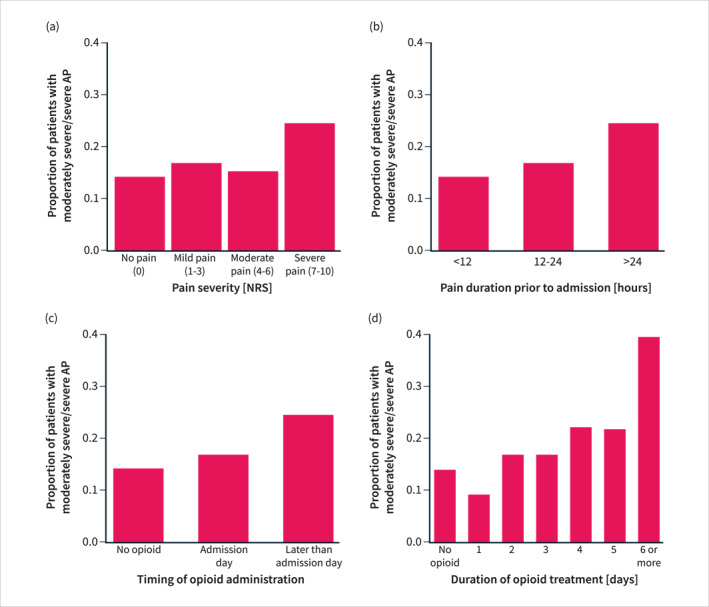
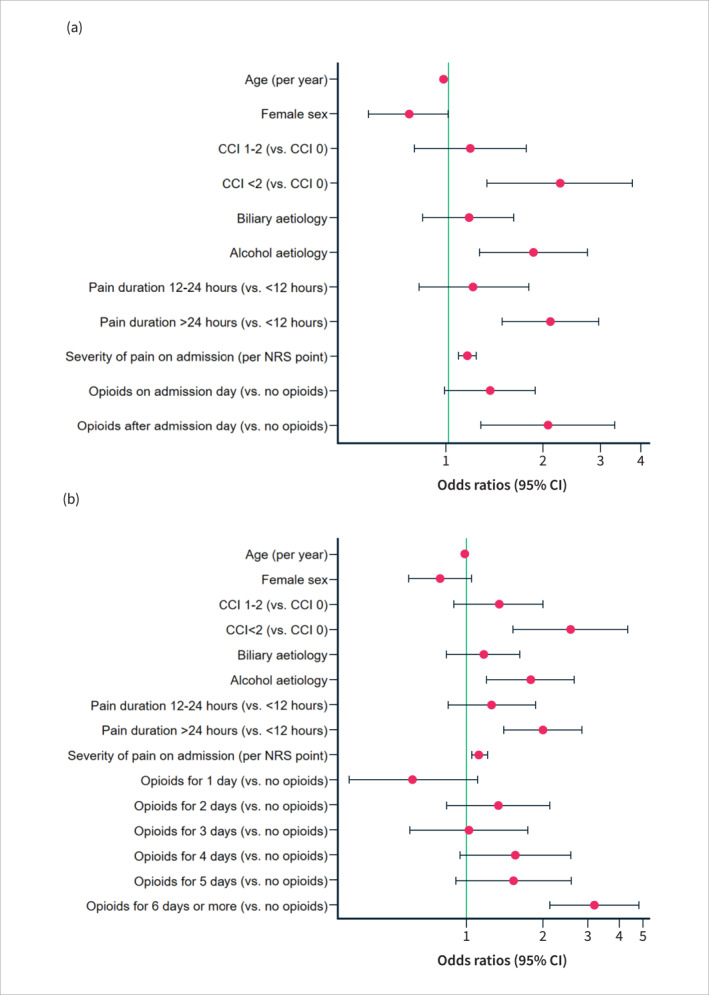
Results: Among a total of 1768 patients, included from 118 centres across 27 countries, 1036 (59%) had opioids administered on admission day, and 167 (9%) received opioids after admission day. On univariate analysis, moderately severe or severe acute pancreatitis was associated with male sex, Asian ethnicity, alcohol aetiology, comorbidity, predicted severe acute pancreatitis, higher pain scores, longer pain duration and opioid treatment (all p < 0.001). On multivariate analysis, comorbidity, alcohol aetiology, longer pain duration and higher pain scores increased the risk of moderately severe or severe acute pancreatitis (all p < 0.001). Furthermore, opioids administered after admission day (but not on admission day) doubled the risk of moderately severe or severe disease (OR 2.07 (95% CI, 1.29-3.33); p = 0.003). Opioid treatment for 6 days or more was an independent risk factor for moderately severe or severe acute pancreatitis (OR 3.21 (95% CI, 2.16-4.79; p < 0.001). On univariate analysis, longer opioid duration was associated with mortality.
Conclusion: Opioid treatment increased the risk of more severe acute pancreatitis only when administered after admission day or for 6 days or more. Future randomised studies should re-evaluate whether opioids might be safe in acute pancreatitis.
Keywords: acute pancreatitis; alcoholic; analgesia; morbidity; mortality; opioid; pain; severity.
© 2024 The Authors. United European Gastroenterology Journal published by Wiley Periodicals LLC on behalf of United European Gastroenterology.
Conflict of interest statement
None to declare.
Figures
Comment in
-
Letter to editor: "opioid analgesia and severity of acute pancreatitis: an international multicentre cohort study on pain management in acute pancreatitis".HPB (Oxford). 2024 Jul;26(7):968. doi: 10.1016/j.hpb.2024.04.006. Epub 2024 Apr 23. HPB (Oxford). 2024. PMID: 38704326 No abstract available.
References
-
- Barlass U, Dutta R, Cheema H, George J, Sareen A, Dixit A, et al. Morphine worsens the severity and prevents pancreatic regeneration in mouse models of acute pancreatitis. Gut. 2018;67(4):600–602. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
