

Cor Triatriatum Dexter With a Sinus Venosus Atrial Septal Defect in a 50-Year-Old Woman: A Case Report
- PMID: 38439997
- PMCID: PMC10910018
- DOI: 10.7759/cureus.53477
Cor Triatriatum Dexter With a Sinus Venosus Atrial Septal Defect in a 50-Year-Old Woman: A Case Report
Abstract
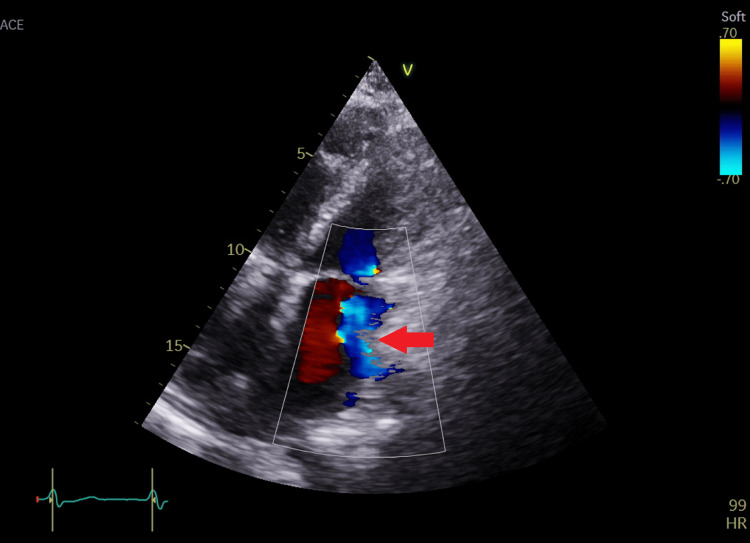
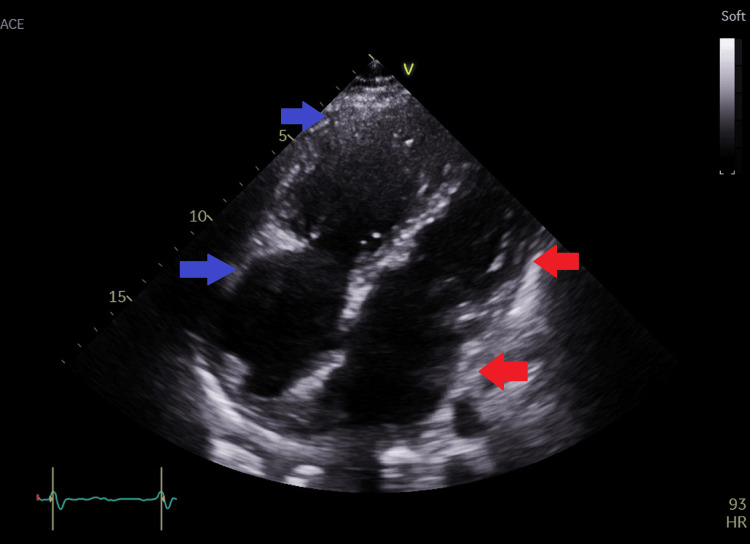
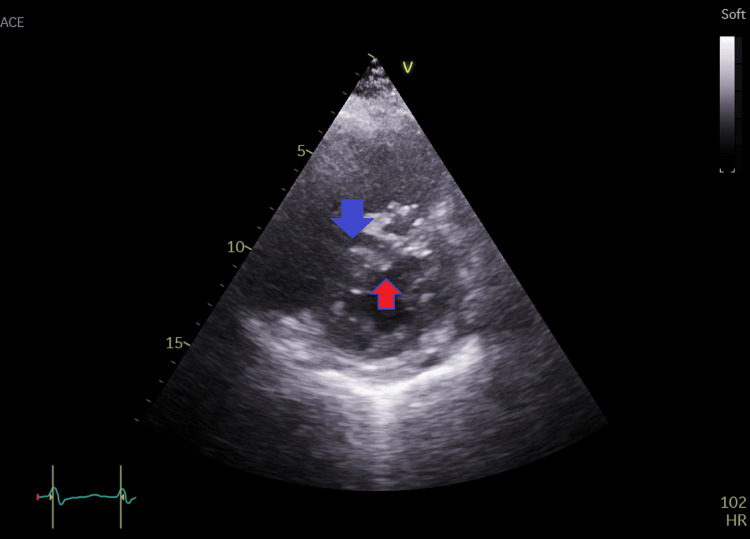
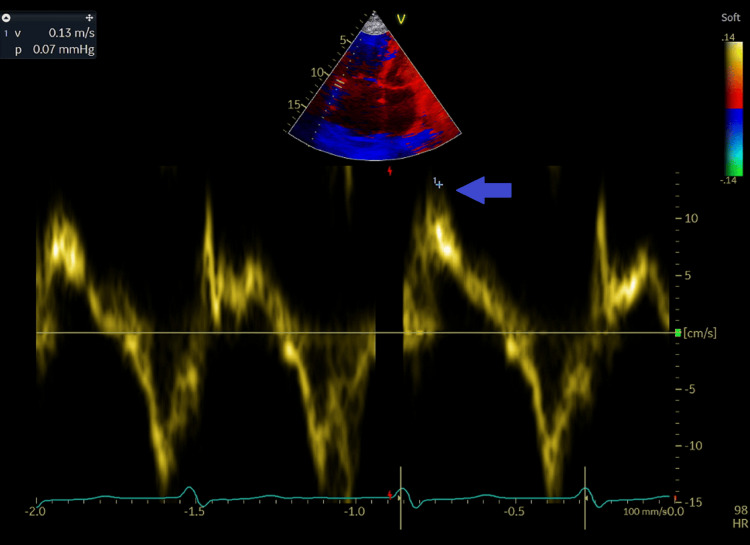
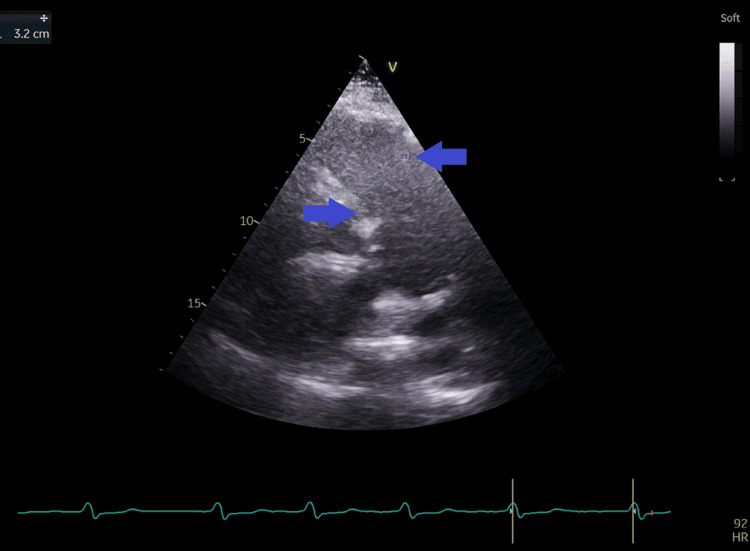
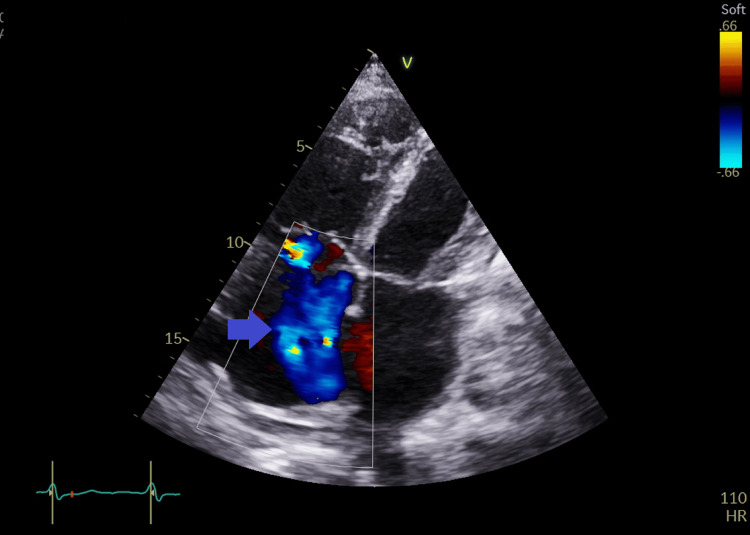
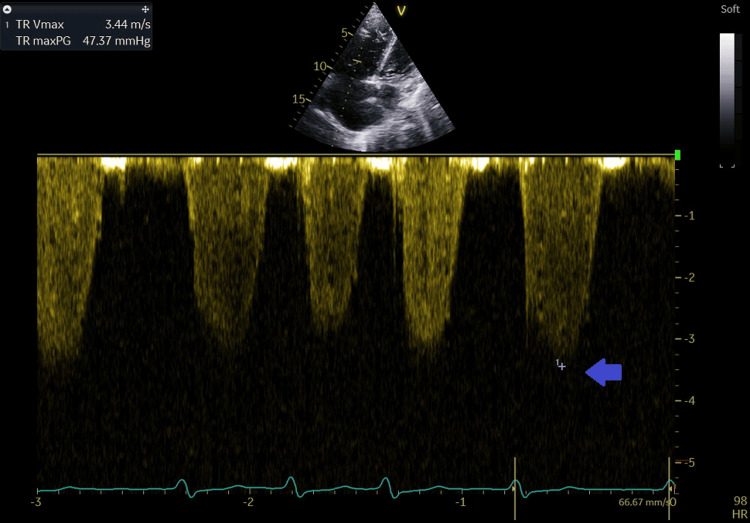
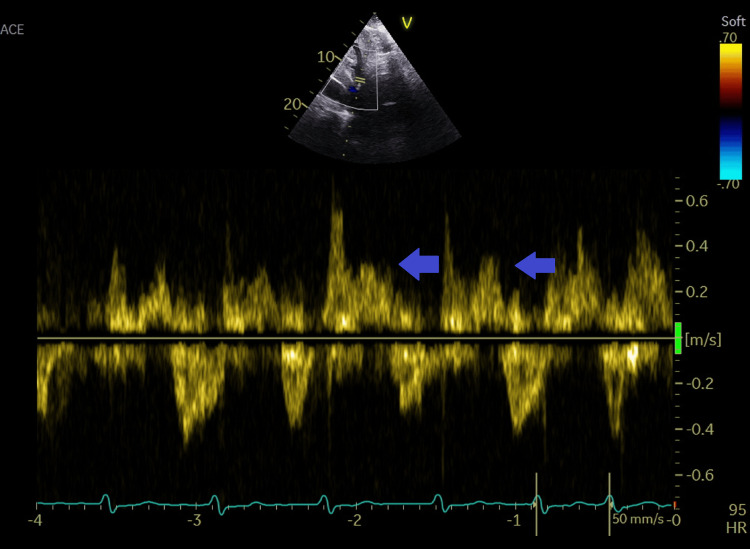
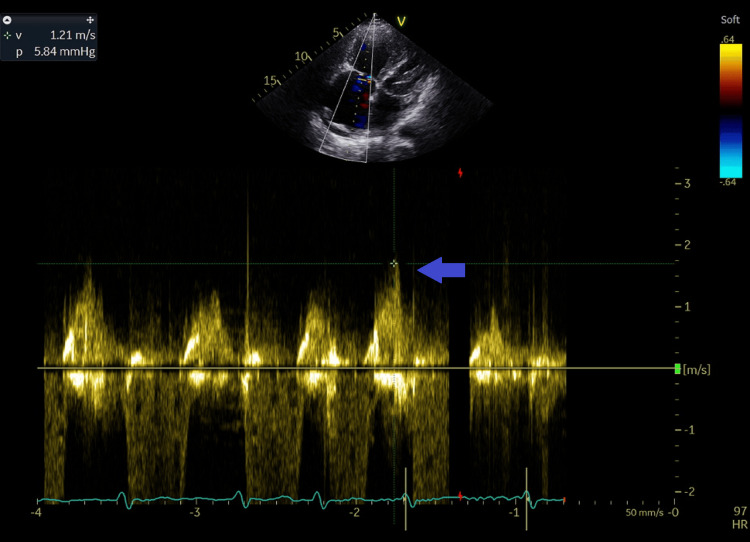
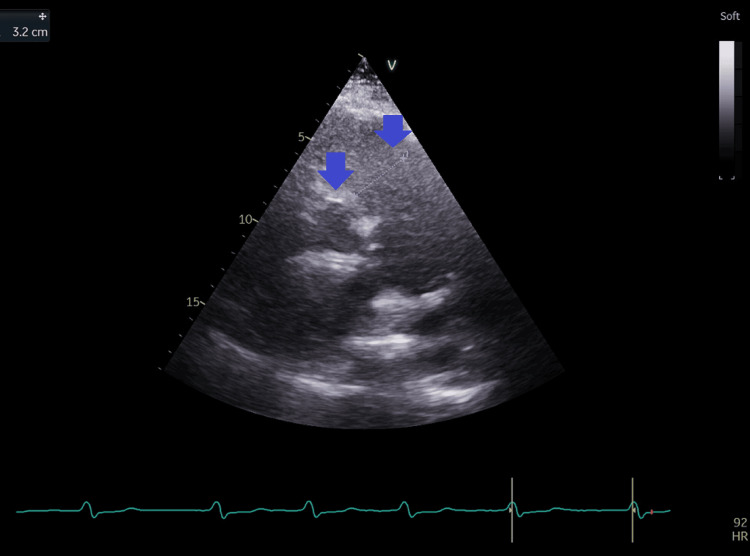
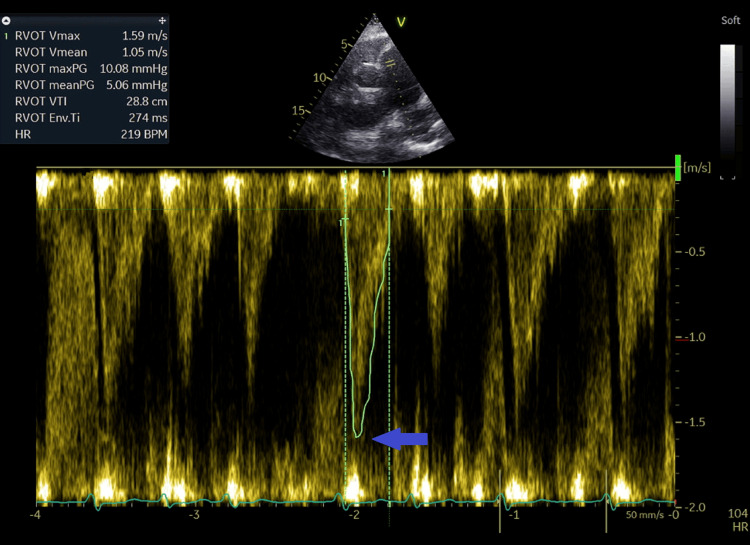
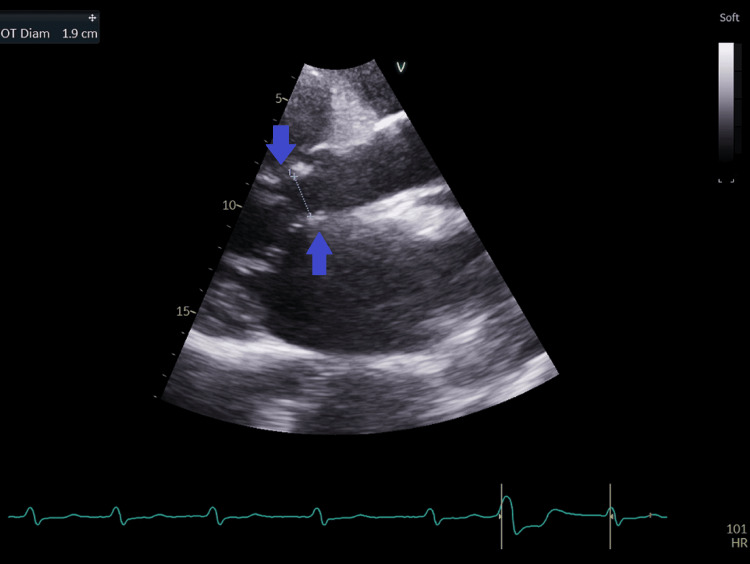
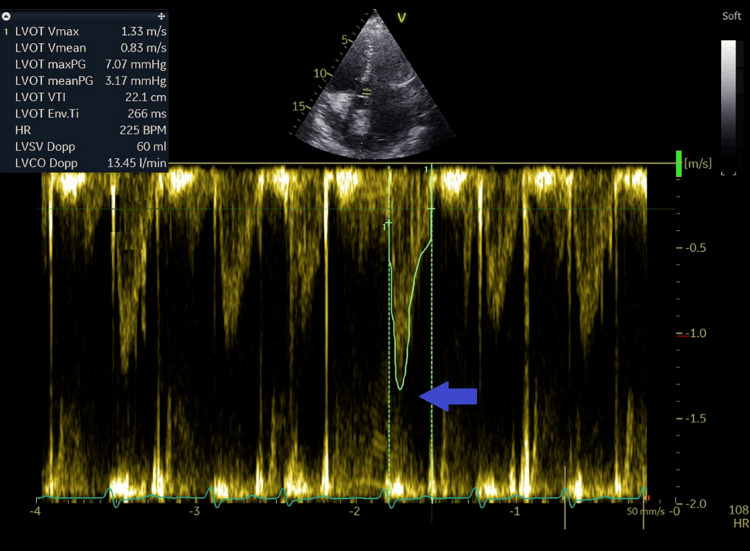
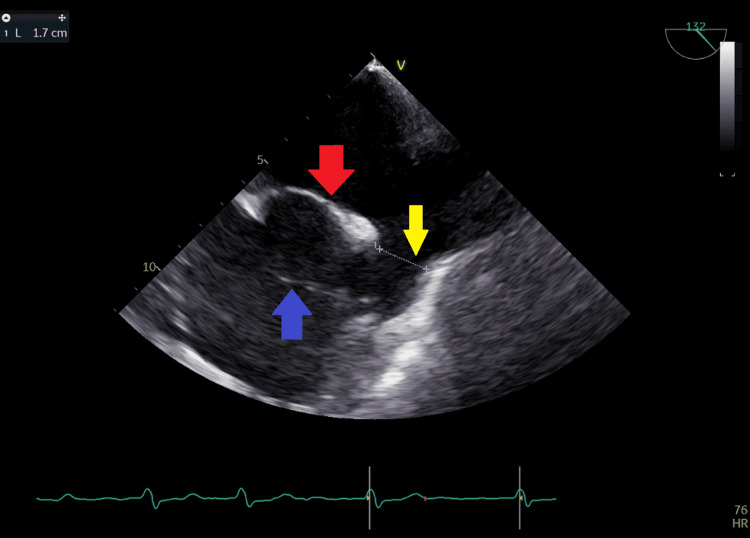
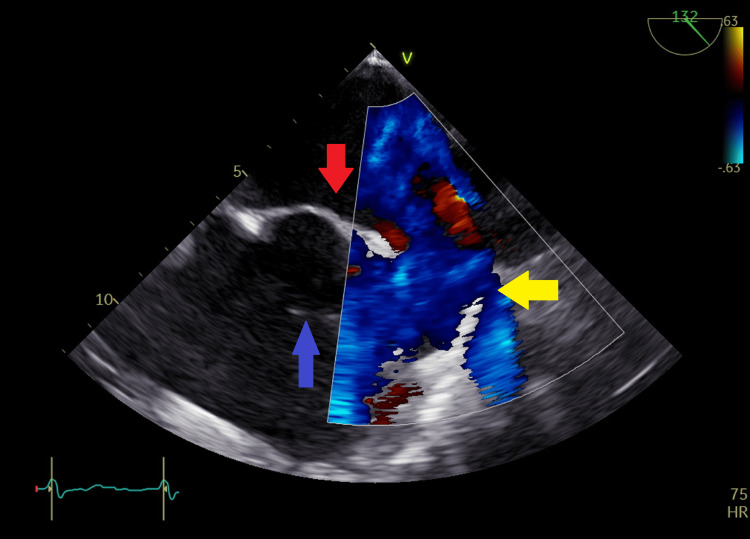
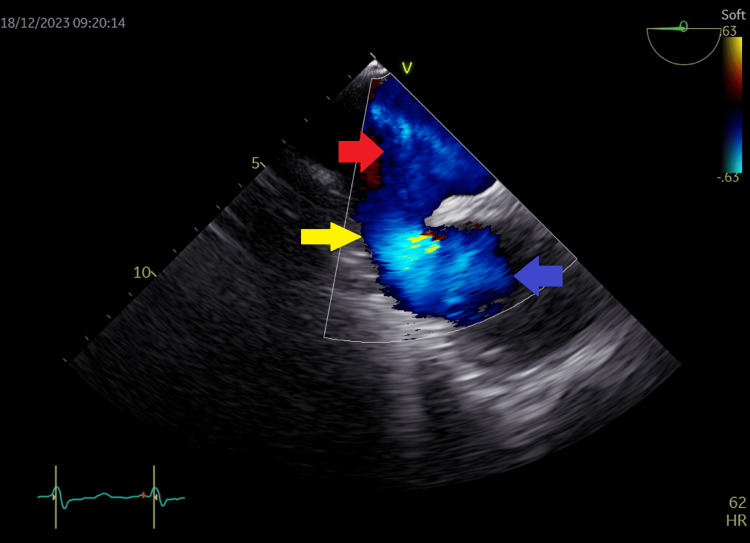
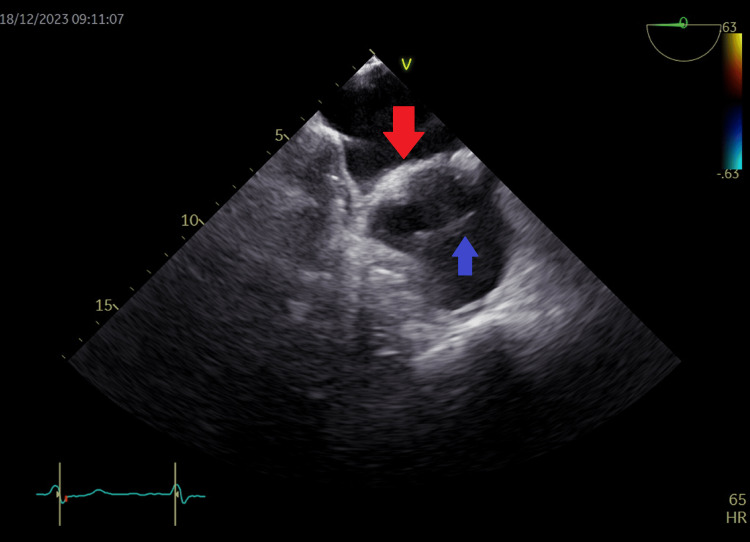
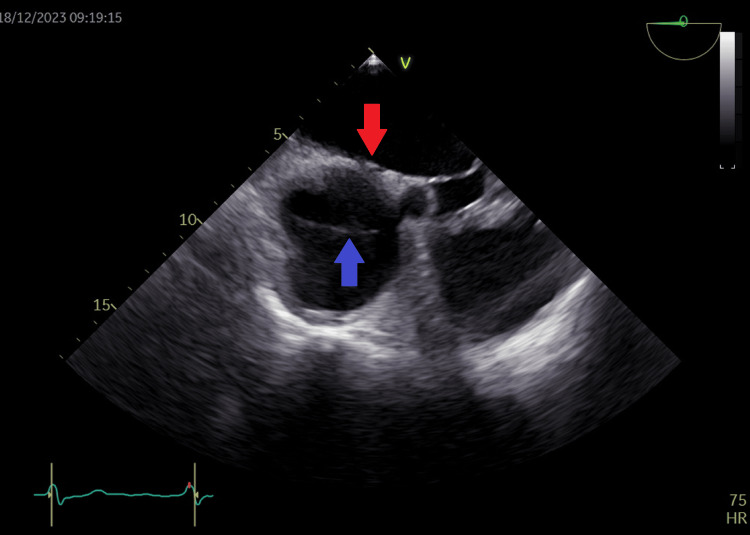
The diagnosis of atrial septal defect (ASD) may be delayed until adulthood or even later in life as it is a well-tolerated congenital heart disease. If patients are not examined and investigated well in childhood, the diagnosis may be delayed until later in adulthood when patients present with palpitations and sometimes dyspnea due to the right chambers dilatation from right ventricular volume overload. In this report, we present a case of a 50-year-old female patient with symptoms of heart failure and atrial fibrillation who was found to have dilated right cardiac chambers, dilated pulmonary artery, severe tricuspid regurgitation, pulmonary hypertension, and a pulmonary-to-systemic flow ratio (Qp/Qs) of more than 1.5 by transthoracic echocardiography and Doppler, indicating left to right shunt at the atrial level. However, transthoracic echocardiography could not visualize the defect, and two-dimensional (2D) transesophageal echocardiography was done in this patient and documented the presence of a sinus venosus ASD with an incomplete cor triatriatum dexter membrane; all four pulmonary veins were identified going to the left atrium. Since the presence of an incomplete cor triatriatum dexter membrane (despite causing no symptoms) makes the percutaneous closure of the sinus venosus ASD and the percutaneous repair of tricuspid regurgitation very difficult, we decided to advise surgical ASD closure and tricuspid valve repair for the patient.
Keywords: adult congenital heart disease; anomalous venous return; atrial septal defects; cor triatriatum dexter; functional tricuspid valve regurgitation; pulmonary hypertension; pulmonary to systemic flow ratio; right cardiac chambers dilatation; sinus venosus atrial septal defect; transthoracic and transesophageal echocardiography.
Copyright © 2024, Kazma et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Atrial septal defect in adulthood: a new paradigm for congenital heart disease. Brida M, Chessa M, Celermajer D, et al. Eur Heart J. 2022;43:2660–2671. - PubMed
-
- Diagnosis of sinus venosus atrial septal defect with transesophageal echocardiography. Pascoe RD, Oh JK, Warnes CA, Danielson GK, Tajik AJ, Seward JB. Circulation. 1996;94:1049–1055. - PubMed
Publication types
LinkOut - more resources
Full Text Sources