

The accuracy of anal self- and companion exams among sexual minority men and transgender women: a prospective analysis
- PMID: 38440068
- PMCID: PMC10910307
- DOI: 10.1016/j.lana.2024.100704
The accuracy of anal self- and companion exams among sexual minority men and transgender women: a prospective analysis
Abstract
Background: Squamous cell carcinoma of the anus (SCCA) annual incidence among sexual minority men with and without HIV is 85/100,000 and 19/100,000 persons, respectively, which is significantly higher than the overall incidence (2/100,000). Incidence may also be higher in transgender women. Since SCCA tumours average ≥30 mm at diagnosis, we assessed the accuracy of individuals to self-detect smaller anal abnormalities.
Methods: Using convenience sampling, the study enrolled sexual minority men and transgender women, aged 25-81 years, in Chicago, Illinois and Houston, Texas, USA, during 2020-2022. Individuals were taught the anal self-examination and anal companion examination (ASE/ACE). Then, a clinician performed a digital anal rectal examination (DARE) before participants conducted the ASE or ACE. The sensitivity, specificity and concordance of the ASE/ACE to detect an abnormality were measured along with factors associated with ASE/ACE and DARE concordance.
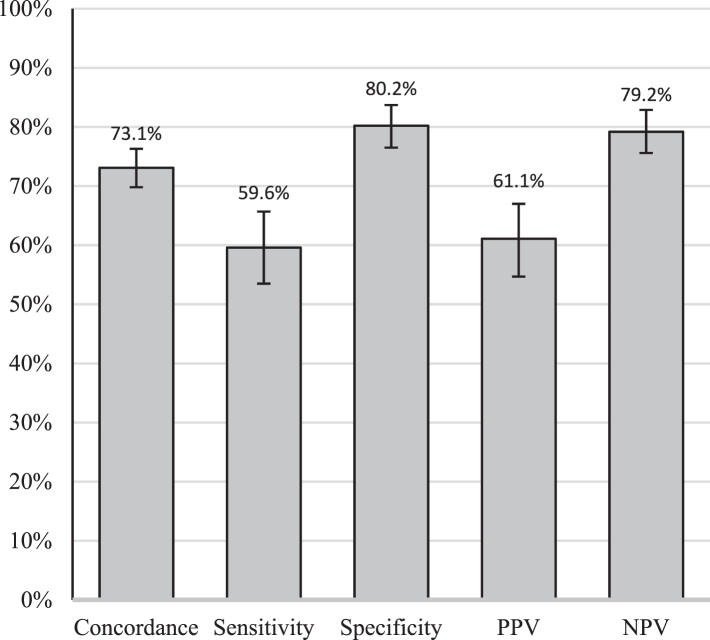
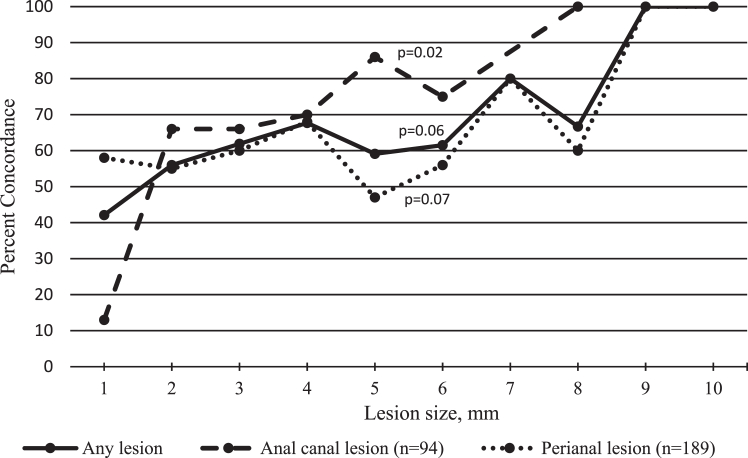
Findings: Among 714 enrolled individuals, the median age was 40 years (interquartile range, 32-54), 36.8% (259/703) were living with HIV, and 47.0% (334/710), 23.4% (166/710), and 23.0% (163/710) were non-Hispanic white, non-Hispanic Black, and Hispanic, respectively. A total of 94.1% (671/713) identified as cisgendered men, and 5.9% (42/713) as gender minorities. A total of 658 participants completed an ASE and 28 couples (56 partners) completed an ACE. Clinicians detected abnormalities in 34.3% (245/714) of individuals. The abnormalities were a median of 3 mm in diameter. Sensitivity and specificity of the ASE/ACE was 59.6% (95% CI 53.5-65.7%) and 80.2% (95% CI 76.6-83.8%), respectively. Overall concordance was 0.73 (95% CI 0.70-0.76) between ASE/ACE and DARE and increased with increasing anal canal lesion size (p = 0.02). Concordance was lower when participants were older and received ASE/ACE training from a lay person rather than a clinician.
Interpretation: Sexual minority men/transgender women may self-detect SCCA when malignant lesions are much smaller than the current mean dimension at presentation of ≥30 mm.
Funding: National Cancer Institute.
Keywords: Anal canal; Anus neoplasms; Digital anal rectal examination; Early detection of cancer; HIV; Homosexuality; Male.
© 2024 The Author(s).
Conflict of interest statement
Aniruddha Hazra declared receiving consulting fees from Gilead Sciences, ViiV Healthcare, and Abbott Technologies; Ashish A. Deshmukh declared receiving consulting fees from Merck Inc., Value Analytics Lab, support to attend EUROGIN, and payment or honoraria for giving talks/conferences at the NIH and Mt. Sinai; Elizabeth Y. Chiao has a leadership or fiduciary role as Chair, solid Tumour Working Group, AIDS Malignancy Consortium; Michael D. Swartz received funding from the NIH.
Figures
Update of
-
The accuracy of anal self- and companion exams among sexual minority men and transgender women: The Prevent Anal Cancer Palpation Study.medRxiv [Preprint]. 2023 Oct 19:2023.10.19.23297209. doi: 10.1101/2023.10.19.23297209. medRxiv. 2023. Update in: Lancet Reg Health Am. 2024 Feb 29;31:100704. doi: 10.1016/j.lana.2024.100704. PMID: 37905024 Free PMC article. Updated. Preprint.
References
-
- Silverberg M.J., Nash R., Becerra-Culqui T.A., et al. Cohort study of cancer risk among insured transgender people. Ann Epidemiol. 2017;27(8):499–501. - PubMed
-
- Centers for Disease Control & Prevention Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1–187. https://www.cdc.gov/std/treatment-guidelines/STI-Guidelines-2021.pdf - PMC - PubMed
-
- Berry J.M., Jay N., Cranston R.D., et al. Progression of anal high-grade squamous intraepithelial lesions to invasive anal cancer among HIV-infected men who have sex with men. Int J Cancer. 2014;134(5):1147–1155. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
