

Subtotal Petrosectomy: Pictorial Review of Clinical Indications and Surgical Approach
- PMID: 38440666
- PMCID: PMC10909040
- DOI: 10.1007/s12070-023-04131-3
Subtotal Petrosectomy: Pictorial Review of Clinical Indications and Surgical Approach
Abstract
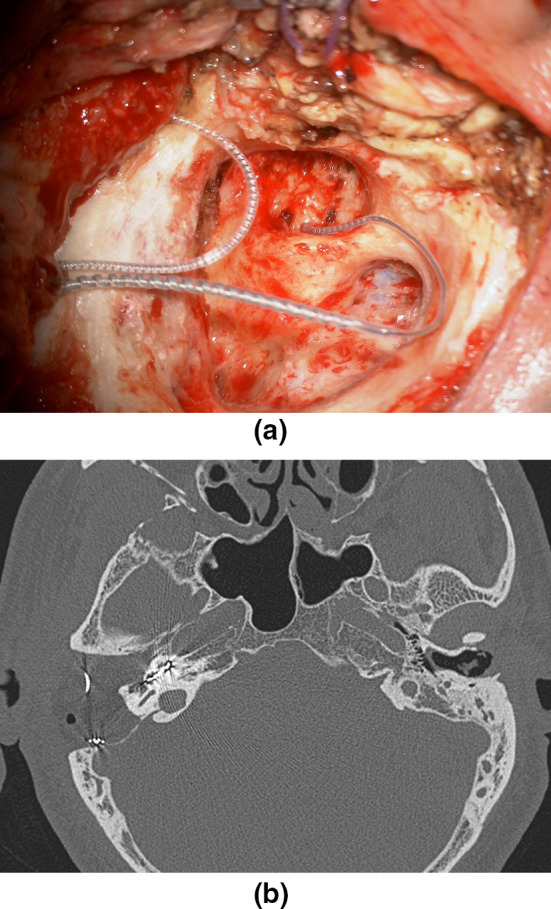
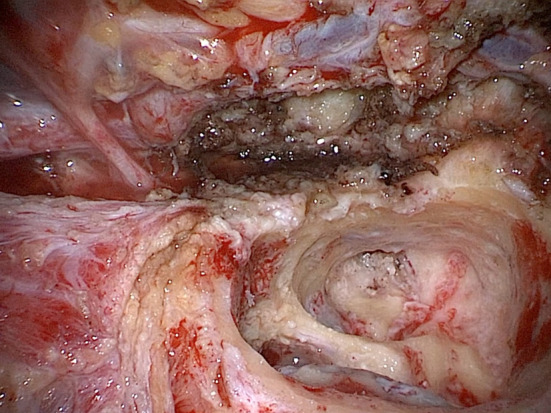
Subtotal petrosectomy (STP) is characterized by obliteration of the middle ear and occlusion of the external auditory canal. The advent of the endoscope has allowed a reduction in morbidity for some conditions such as cholesteatoma and other middle ear disorders, but STP still plays an important role. A retrospective review of medical records and videos of patients who had undergone STP was performed. Perioperative data and images were collected from various clinical cases who had undergone subtotal petrosectomy at our tertiary referral university hospital in Verona. We confronted our experience with a review of the literature to present the main indications for this type of procedure. STP allows a variety of diseases to be managed effectively as it offers the possibility of a definitive healing with radical clearance of temporal bone. Moreover, it can be safely combined with other procedures with a very low complication rate. Although the endoscope represents a revolution in ear surgery, STP, when indicated, is nowadays a surgical option that should be included in the otosurgeon's portfolio.
Keywords: Cholesteatoma; Cochlear implant; Skull base tumors; Subtotal petrosectomy; Temporal bone fractures.
© Association of Otolaryngologists of India 2023. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Conflict of interestAll the authors declare that they have no conflict of interest.
Figures







References
-
- Fisch U. Microsurgery of the skull base. Stuttgart: Georg Thieme Verlag; 1988.
LinkOut - more resources
Full Text Sources