

Pharmacokinetics and exposure-safety relationship of ciprofol for sedation in mechanically ventilated patients in the intensive care unit
- PMID: 38440939
- PMCID: PMC11098162
- DOI: 10.1002/psp4.13121
Pharmacokinetics and exposure-safety relationship of ciprofol for sedation in mechanically ventilated patients in the intensive care unit
Abstract
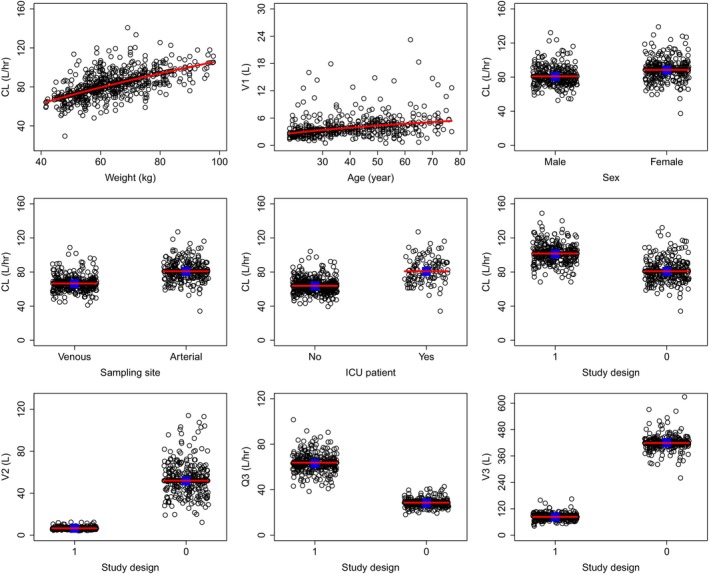
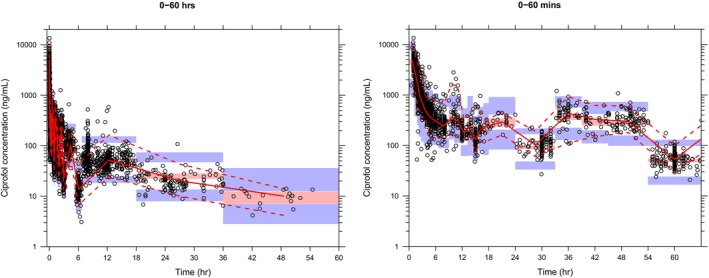
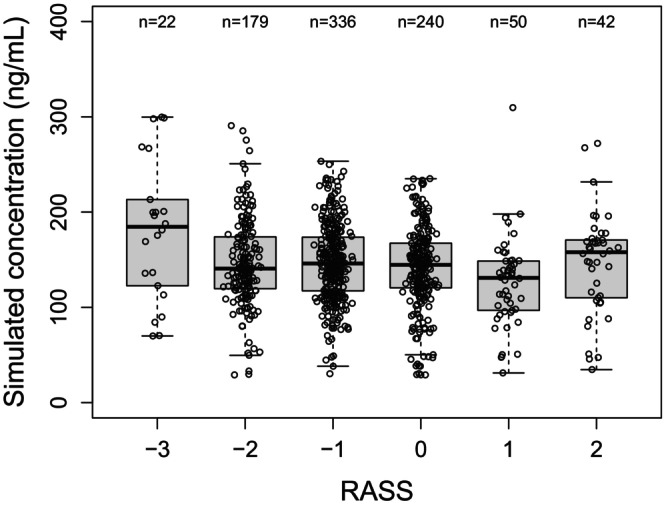
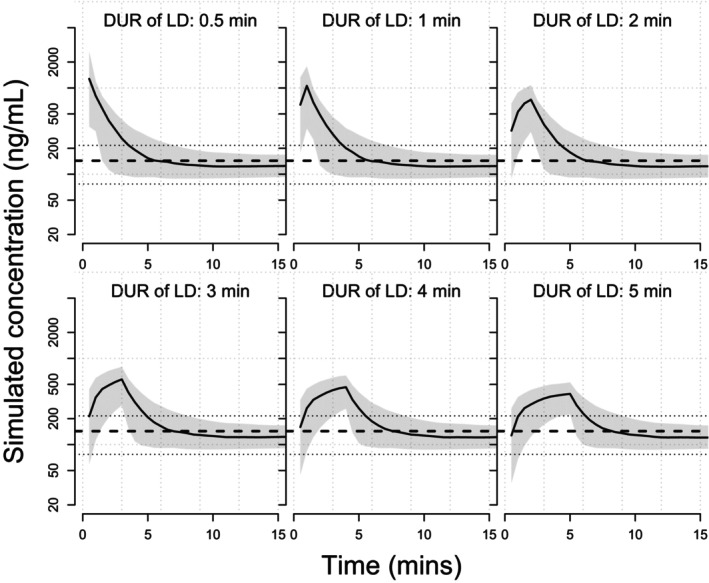
Ciprofol (HSK3486) is a newly developed, highly selective γ-aminobutyric acid-A (GABAA) receptor potentiator that is recently approved for a new indication of sedation for patients in the intensive care unit (ICU) in China. This analysis aimed to characterize the population pharmacokinetics (PopPKs) of ciprofol and evaluate the relationship of exposure with hypotension in mechanically ventilated patients in the ICU. A total of 462 subjects with 3918 concentration measurements from two clinical trials of mechanically ventilated patients in the ICU, four clinical trials of elective surgical patients, and six clinical trials of healthy subjects were used in the PopPK analysis. Exposure-safety relationship for hypotension was evaluated based on the data gathered from 112 subjects in two clinical trials of mechanically ventilated patients in the ICU. Ciprofol pharmacokinetics (PKs) was adequately described by a three-compartment linear disposition model with first-order elimination. Body weight, age, sex, blood sampling site (vein vs. arterial), study design (long-term infusion vs. short-term infusion), and patient population (ICU vs. non-ICU) were identified as statistically significant covariates on the PKs of ciprofol. Within the exposure range of the mechanically ventilated ICU patient population, no meaningful association was observed between ciprofol exposure and the incidence of hypotension. These results support the dosing regimen currently used in mechanically ventilated patients in the ICU.
© 2024 The Authors. CPT: Pharmacometrics & Systems Pharmacology published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
As of the date of submission of this manuscript, L.L. and X.X. declare no potential conflicts of interest. K.W. and Z.S. are employees of Shanghai Qiangshi Information Technology Co., Ltd. and served as consultants for Haisco Pharmaceutical Group Co. Ltd. P.Y., N.W., M.H., X.L., and M.C. are employees of Haisco Pharmaceutical Group Co. Ltd.
Figures
Similar articles
-
Ciprofol versus propofol for long-term sedation in mechanically ventilated patients with sepsis: a randomized controlled trial.BMC Anesthesiol. 2025 Apr 9;25(1):161. doi: 10.1186/s12871-025-03042-w. BMC Anesthesiol. 2025. PMID: 40205333 Free PMC article. Clinical Trial.
-
Efficacy and safety of ciprofol for long-term sedation in patients receiving mechanical ventilation in ICUs: a prospective, single-center, double-blind, randomized controlled protocol.Front Pharmacol. 2023 Aug 21;14:1235709. doi: 10.3389/fphar.2023.1235709. eCollection 2023. Front Pharmacol. 2023. PMID: 37670942 Free PMC article.
-
Population pharmacokinetic/pharmacodynamic modeling and exposure-response analysis of ciprofol in the induction and maintenance of general anesthesia in patients undergoing elective surgery: A prospective dose optimization study.J Clin Anesth. 2024 Feb;92:111317. doi: 10.1016/j.jclinane.2023.111317. Epub 2023 Nov 15. J Clin Anesth. 2024. PMID: 37976683
-
Dexmedetomidine vs other sedatives in critically ill mechanically ventilated adults: a systematic review and meta-analysis of randomized trials.Intensive Care Med. 2022 Jul;48(7):811-840. doi: 10.1007/s00134-022-06712-2. Epub 2022 Jun 1. Intensive Care Med. 2022. PMID: 35648198
-
Protocol-directed sedation versus non-protocol-directed sedation in mechanically ventilated intensive care adults and children.Cochrane Database Syst Rev. 2018 Nov 12;11(11):CD009771. doi: 10.1002/14651858.CD009771.pub3. Cochrane Database Syst Rev. 2018. PMID: 30480753 Free PMC article.
Cited by
-
Ciprofol prevents ferroptosis in LPS induced acute lung injury by activating the Nrf2 signaling pathway.BMC Pulm Med. 2024 Nov 28;24(1):591. doi: 10.1186/s12890-024-03415-w. BMC Pulm Med. 2024. PMID: 39609781 Free PMC article.
-
Effects of cipepofol on breathing patterns, respiratory drive, and inspiratory effort in mechanically ventilated patients.Front Med (Lausanne). 2025 Feb 25;12:1539238. doi: 10.3389/fmed.2025.1539238. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40070647 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
