

Primary non-refluxing megaureter: Natural history, follow-up and treatment
- PMID: 38441661
- PMCID: PMC11035438
- DOI: 10.1007/s00431-024-05494-7
Primary non-refluxing megaureter: Natural history, follow-up and treatment
Abstract
Primary non-refluxing megaureter (PMU) is a congenital dilation of the ureter which is not related to vesicoureteral reflux, duplicated collecting systems, ureterocele, ectopic ureter, or posterior urethral valves and accounts for 5 to 10% of all prenatal hydronephrosis (HN) cases. The etiology is a dysfunction or stenosis of the distal ureter. Most often PMU remains asymptomatic with spontaneous resolution allowing for non-operative management. Nevertheless, in selective cases such as the development of febrile urinary tract infections, worsening of the ureteral dilatation, or reduction in relative renal function, surgery should be considered.
Conclusion: Ureteral replantation with excision of the dysfunctional ureteral segment and often ureteral tapering is the gold-standard procedure for PMU, although endoscopic treatment has been shown to have a fair success rate in many studies. In this review, we discuss the natural history, follow-up, and treatment of PMU.
What is known: • PMU is the result of an atonic or stenotic segment of the distal ureter, resulting in congenital dilation of the ureter, and is frequently diagnosed on routine antenatal ultrasound.
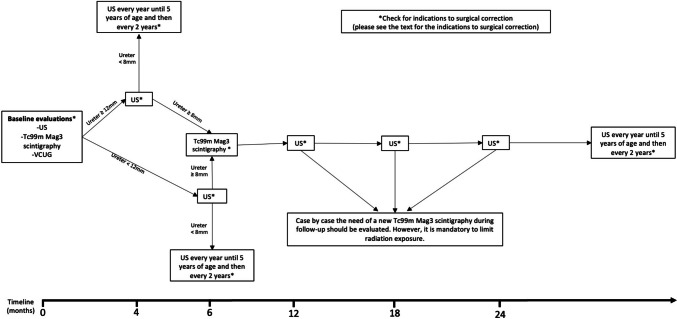
What is new: • Most often, PMU remains asymptomatic and clinically stable, allowing for non-operative management. • Nevertheless, since symptoms can appear even after years of observation, long-term ultrasound follow-up is recommended, even up to young adulthood, if hydroureteronephrosis persists. • Ureteral replantation is the gold standard in case surgery is needed. In selected cases, however, HPBD could be a reasonable alternative.
Keywords: Continuous antibiotic prophylaxis; High-pressure balloon dilation; Primary non-refluxing megaureter; Ureteral replantation; Urinary tract infections.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Endoscopic treatment of primary obstructive megaureter with high pressure balloon dilation in infants.J Pediatr Urol. 2024 Feb;20(1):67-74. doi: 10.1016/j.jpurol.2023.09.007. Epub 2023 Sep 16. J Pediatr Urol. 2024. PMID: 37783596
-
Treatment of the neonatal and infant megaureter in reflux, obstruction and complex congenital anomalies.Acta Urol Belg. 1997 Jun;65(2):45-7. Acta Urol Belg. 1997. PMID: 9287434
-
Refluxing ureteral reimplantation: a logical method for managing neonatal UVJ obstruction.J Pediatr Urol. 2014 Oct;10(5):824-30. doi: 10.1016/j.jpurol.2014.01.027. Epub 2014 Feb 28. J Pediatr Urol. 2014. PMID: 24850437
-
British Association of Paediatric Urologists consensus statement on the management of the primary obstructive megaureter.J Pediatr Urol. 2014 Feb;10(1):26-33. doi: 10.1016/j.jpurol.2013.09.018. Epub 2013 Oct 16. J Pediatr Urol. 2014. PMID: 24206785
-
Megaureter: classification, pathophysiology, and management.Pediatr Med Chir. 2000;22(1):15-24. Pediatr Med Chir. 2000. PMID: 11387761 Review. English, Italian.
Cited by
-
Predictive Factors for Spontaneous Resolution in Primary Obstructive Megaureter: The Impact of Hydronephrosis Severity on Clinical Outcomes.J Clin Med. 2025 Apr 4;14(7):2463. doi: 10.3390/jcm14072463. J Clin Med. 2025. PMID: 40217912 Free PMC article.
-
Case Report: Prolonged survival in Schinzel-Giedion syndrome featuring megaureter and de novo SETBP1 mutation.Front Pediatr. 2025 Mar 7;13:1534192. doi: 10.3389/fped.2025.1534192. eCollection 2025. Front Pediatr. 2025. PMID: 40123672 Free PMC article.
-
Non-contrast cine magnetic resonance urography in evaluating and monitoring of primary obstructive megaureter: a case series study.Abdom Radiol (NY). 2025 Apr 11. doi: 10.1007/s00261-025-04938-4. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40214700
References
-
- Joseph DB (2010) Ureterovesical junction anomalies: Megaureters. In: Gearhart JP, Rink RC, Mouriquand PDE (eds) Pediatr Urol, 2nd ed. Elsevier, pp 272–282. 10.1016/B978-1-4160-3204-5.00021-9
-
- Smith ED. Report of working party to establish an international nomenclature for the large ureter. Birth Defects Orig Artic Ser. 1977;13(5):3–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
