

VEGF-C prophylaxis favors lymphatic drainage and modulates neuroinflammation in a stroke model
- PMID: 38442272
- PMCID: PMC10913814
- DOI: 10.1084/jem.20221983
VEGF-C prophylaxis favors lymphatic drainage and modulates neuroinflammation in a stroke model
Abstract
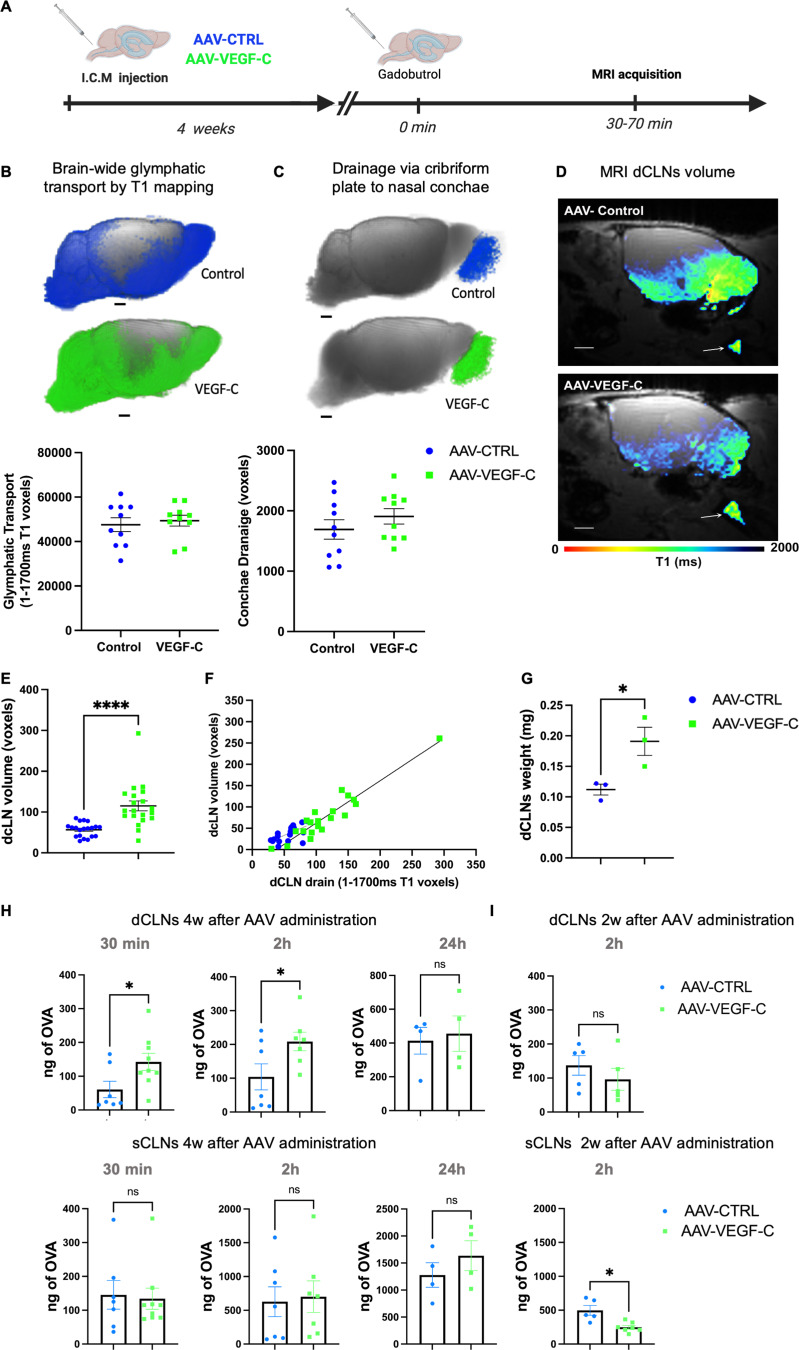
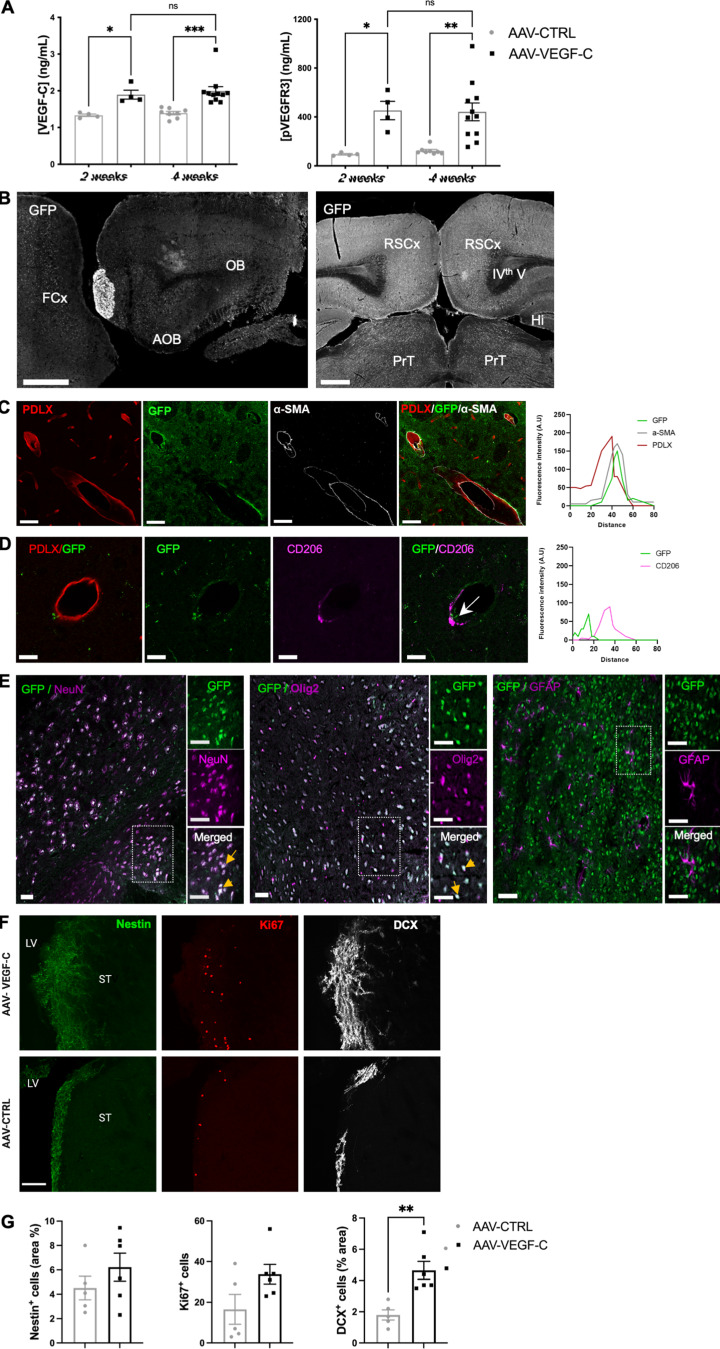
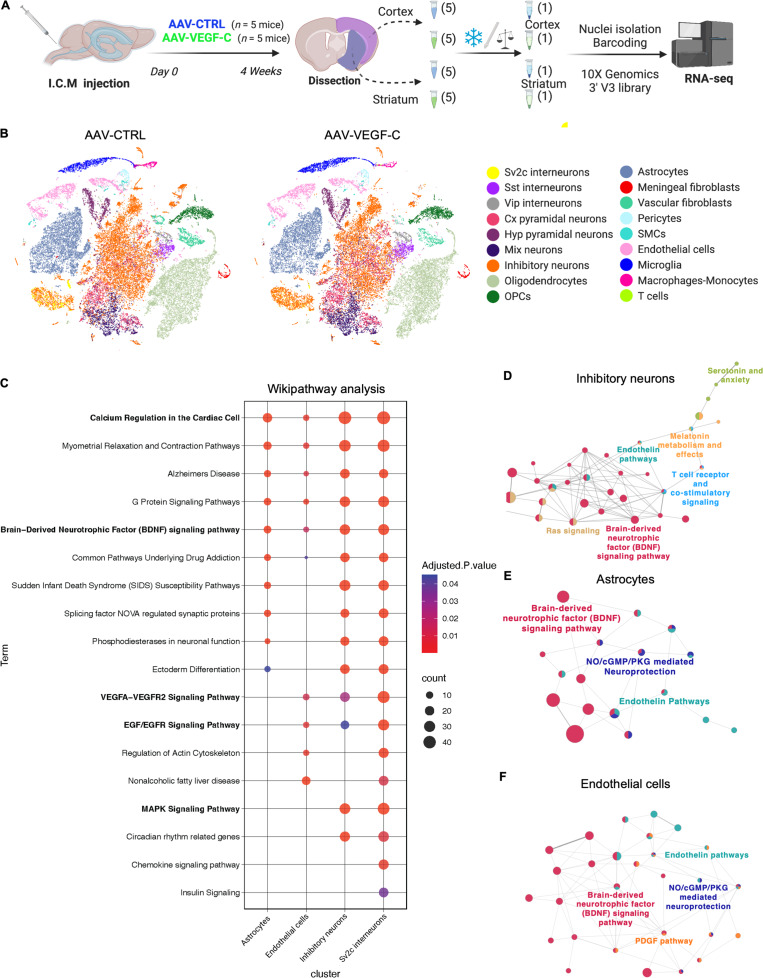
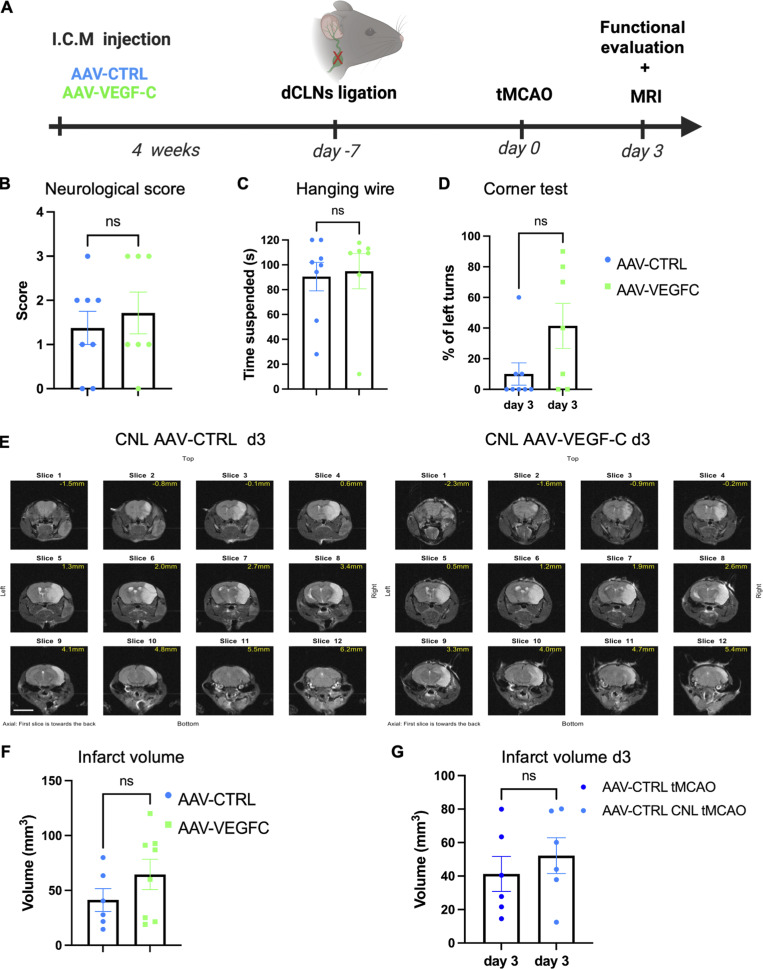
Meningeal lymphatic vessels (MLVs) promote tissue clearance and immune surveillance in the central nervous system (CNS). Vascular endothelial growth factor-C (VEGF-C) regulates MLV development and maintenance and has therapeutic potential for treating neurological disorders. Herein, we investigated the effects of VEGF-C overexpression on brain fluid drainage and ischemic stroke outcomes in mice. Intracerebrospinal administration of an adeno-associated virus expressing mouse full-length VEGF-C (AAV-mVEGF-C) increased CSF drainage to the deep cervical lymph nodes (dCLNs) by enhancing lymphatic growth and upregulated neuroprotective signaling pathways identified by single nuclei RNA sequencing of brain cells. In a mouse model of ischemic stroke, AAV-mVEGF-C pretreatment reduced stroke injury and ameliorated motor performances in the subacute stage, associated with mitigated microglia-mediated inflammation and increased BDNF signaling in brain cells. Neuroprotective effects of VEGF-C were lost upon cauterization of the dCLN afferent lymphatics and not mimicked by acute post-stroke VEGF-C injection. We conclude that VEGF-C prophylaxis promotes multiple vascular, immune, and neural responses that culminate in a protection against neurological damage in acute ischemic stroke.
© 2024 Boisserand et al.
Conflict of interest statement
Disclosures: H. Benveniste reported grants from National Center for Complementary and Integrative Health 1R01AT011419 outside the submitted work. F. Hyder reported being the founder and having an equity interest in of InnovaCyclics LLC, which is a biotechnology company creating next-gen MRI contrast agents that has licensed several IPs in biocompatible smart MRI probes comprised of transition metals that are biomarkers of H+/Na+ imbalances within tumor microenvironment, which are linked to proliferative and invasive phenotypes, and thereby, bypass the need for invasive biopsies. J.-L. Thomas reported grants from the French National Research Agency during the conduct of the study and personal fees from Springer-Nature outside the submitted work; in addition, J.-L. Thomas had a patent to Increasing lymphatics for brain tumor therapy with royalties paid. No other disclosures were reported.
Figures











Comment in
-
Meningeal lymphatics can influence stroke outcome.J Exp Med. 2024 Apr 1;221(4):e20232305. doi: 10.1084/jem.20232305. Epub 2024 Mar 5. J Exp Med. 2024. PMID: 38442271 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
