

Comparative efficacy and safety of different anti-VEGF agents combined with different delivery methods for neovascular glaucoma: a systematic review and Bayesian network meta-analysis
- PMID: 38443085
- PMCID: PMC11146364
- DOI: 10.1136/bmjopen-2023-080103
Comparative efficacy and safety of different anti-VEGF agents combined with different delivery methods for neovascular glaucoma: a systematic review and Bayesian network meta-analysis
Abstract
Objective: To compare the efficacy and safety of different anti-vascular endothelial growth factor (VEGF) agents combined with different delivery methods for neovascular glaucoma (NVG).
Design: Systematic review and Bayesian network meta-analysis (NMA).
Data sources: PubMed, Embase, Cochrane Library, Web of Science, ClinicalTrials.gov, ISRCTN and Chinese databases including the China National Knowledge Infrastructure, China Science Periodical Database (Wanfang Database), VIP Journal Integration Platform and China Biology Medicine Database were searched from inception to 5 September 2022.
Eligibility criteria: We included randomised controlled trials (RCTs) that investigated the treatment of NVG using different anti-VEGF agents combined with various methods of drug administration, without any language limitations. All patients included underwent panretinal laser photocoagulation and there were no restrictions on prior glaucoma surgery.
Data extraction and synthesis: Two independent reviewers extracted data and assessed the risk of bias. Random-effect Bayesian NMA was conducted to compare the efficacy and safety and rank priority of anti-VEGF regimens. The source of heterogeneity and the related factors affecting the stability of the results were also explored. CINeMA (Confidence in Network Meta-Analysis) was used to assess the certainty of evidence.
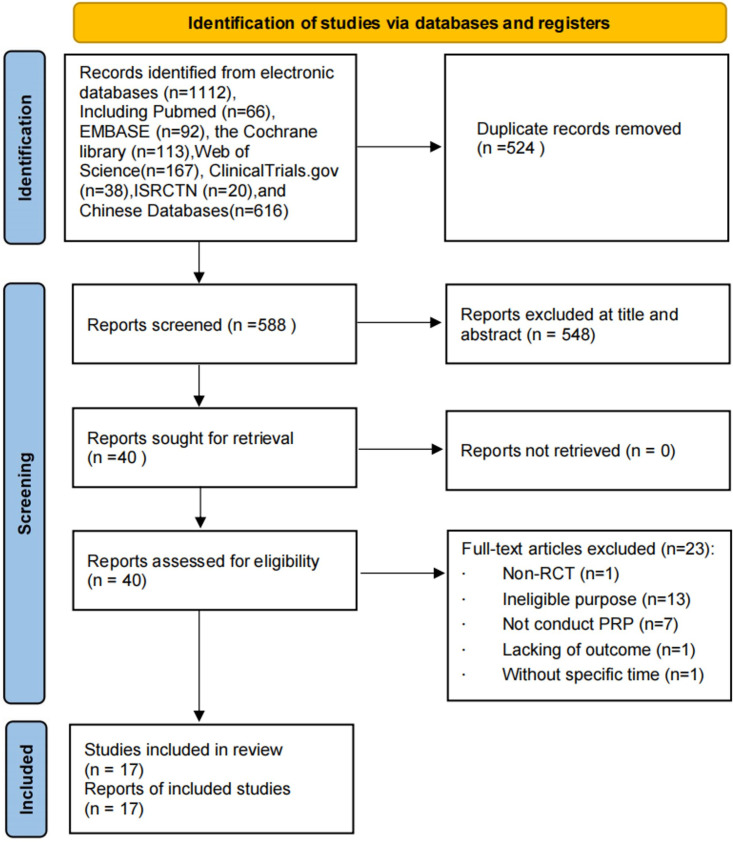
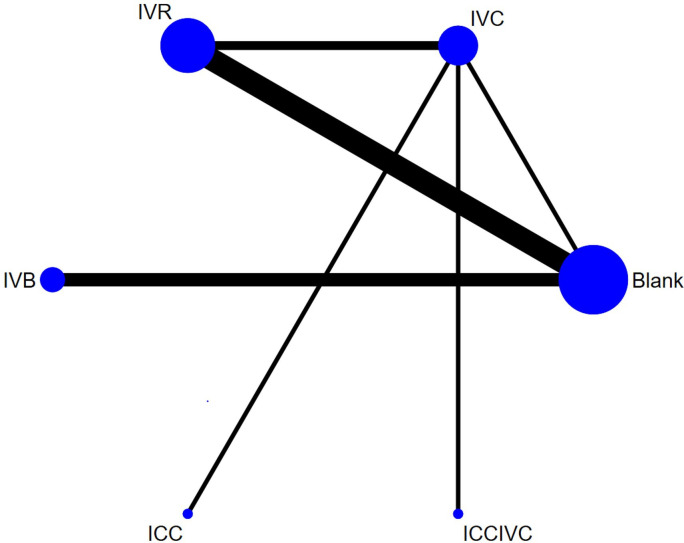
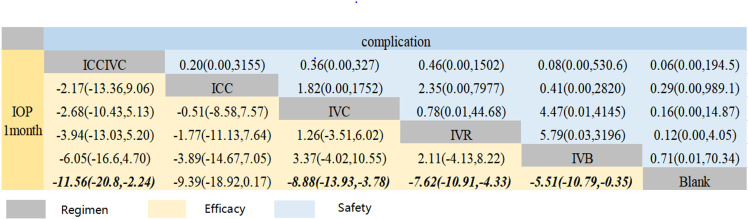
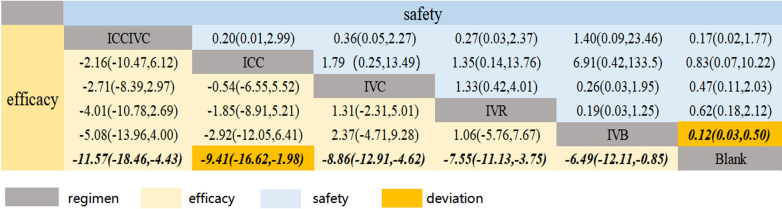
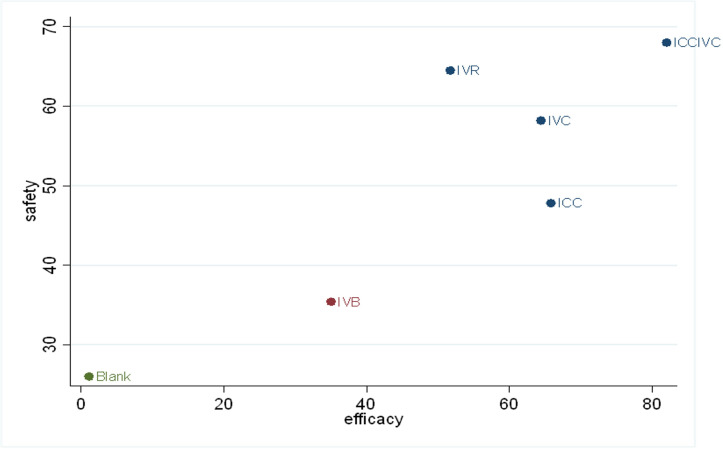
Results: Our analysis included 17 RCTs involving a total of 1311 eyes from 1228 patients. We examined five different treatment regimens, which used three different anti-VEGF drugs. The following treatments showed a significant decrease in intraocular pressure (IOP) compared with the control group at 1 month after glaucoma surgery: simultaneous intravitreal and intracameral injection of conbercept (ICCIVC) (mean difference (MD)=-11.56, 95% credible interval (CrI) -20.8 to -2.24), intravitreal injection of conbercept (MD=-8.88, 95% CrI -13.93 to -3.78), intravitreal injection of ranibizumab (MD=-7.62, 95% CrI -10.91 to -4.33) and intravitreal injection of bevacizumab IVB) (MD=-5.51, 95% CrI -10.79 to -0.35). The surface under the cumulative ranking curve (SUCRA) analysis indicated that ICCIVC (82.0%) may be the most effective regimen in reducing IOP. In terms of safety, there were no statistically significant differences among the interventions. According to the SUCRA analysis, ICCIVC (68.0%) was considered the safest choice with the fewest complications. Subgroup and meta-regression analyses showed that mean age was the main source of heterogeneity. Sensitivity analysis demonstrated the robustness of the study results.
Conclusion: ICCIVC was more effective and safer than other anti-VEGF regimens for NVG. Simultaneous intravitreal and intracameral injection was found to be the best route of administration, and conbercept was found to be the superior drug selection when compared with ranibizumab and bevacizumab.
Prospero registration number: CRD42022309676.
Keywords: Glaucoma; Medical ophthalmology; Ophthalmology.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical