

Comparing anti-tumor and anti-self immunity in a patient with melanoma receiving immune checkpoint blockade
- PMID: 38443917
- PMCID: PMC10916264
- DOI: 10.1186/s12967-024-04973-7
Comparing anti-tumor and anti-self immunity in a patient with melanoma receiving immune checkpoint blockade
Abstract
Background: Tumor regression following immune checkpoint blockade (ICB) is often associated with immune-related adverse events (irAEs), marked by inflammation in non-cancerous tissues. This study was undertaken to investigate the functional relationship between anti-tumor and anti-self immunity, to facilitate irAE management while promoting anti-tumor immunity.
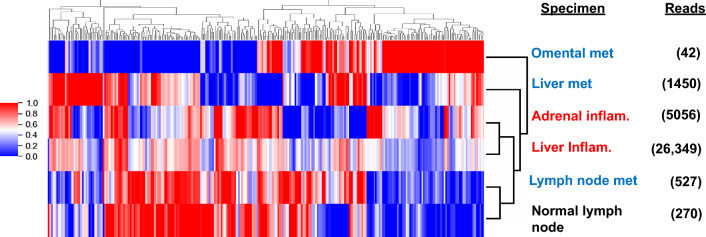
Methods: Multiple biopsies from tumor and inflamed tissues were collected from a patient with melanoma experiencing both tumor regression and irAEs on ICB, who underwent rapid autopsy. Immune cells infiltrating melanoma lesions and inflamed normal tissues were subjected to gene expression profiling with multiplex qRT-PCR for 122 candidate genes. Subsequently, immunohistochemistry was conducted to assess the expression of 14 candidate markers of immune cell subsets and checkpoints. TCR-beta sequencing was used to explore T cell clonal repertoires across specimens.
Results: While genes involved in MHC I/II antigen presentation, IFN signaling, innate immunity and immunosuppression were abundantly expressed across specimens, irAE tissues over-expressed certain genes associated with immunosuppression (CSF1R, IL10RA, IL27/EBI3, FOXP3, KLRG1, SOCS1, TGFB1), including those in the COX-2/PGE2 pathway (IL1B, PTGER1/EP1 and PTGER4/EP4). Immunohistochemistry revealed similar proportions of immunosuppressive cell subsets and checkpoint molecules across samples. TCRseq did not indicate common TCR repertoires across tumor and inflammation sites, arguing against shared antigen recognition between anti-tumor and anti-self immunity in this patient.
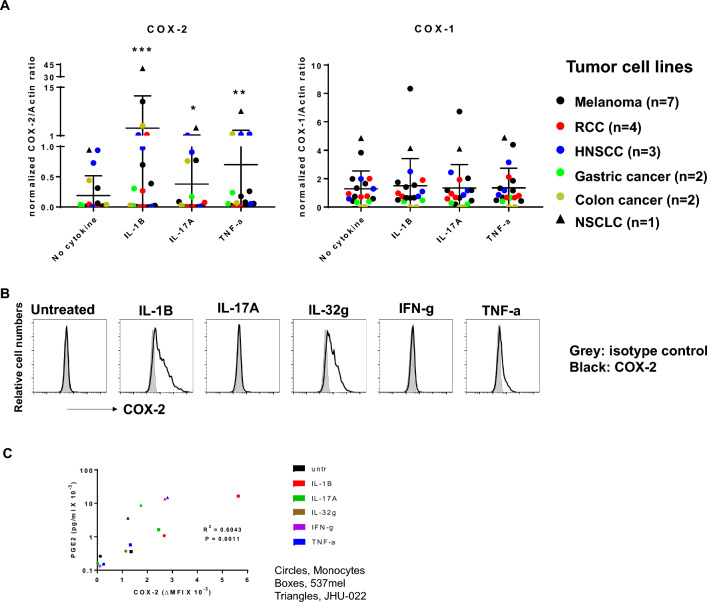
Conclusions: This comprehensive study of a single patient with melanoma experiencing both tumor regression and irAEs on ICB explores the immune landscape across these tissues, revealing similarities between anti-tumor and anti-self immunity. Further, it highlights expression of the COX-2/PGE2 pathway, which is known to be immunosuppressive and potentially mediates ICB resistance. Ongoing clinical trials of COX-2/PGE2 pathway inhibitors targeting the major COX-2 inducer IL-1B, COX-2 itself, or the PGE2 receptors EP2 and EP4 present new opportunities to promote anti-tumor activity, but may also have the potential to enhance the severity of ICB-induced irAEs.
Keywords: COX-2; Gene expression profiling (GEP); Immune checkpoint blockade (ICB); Immune related adverse events (irAEs); Melanoma; Rapid autopsy; Tumor infiltrating lymphocytes (TILs).
© 2024. The Author(s).
Conflict of interest statement
LCC is a consultant for Amgen, Bristol Myers Squibb, and Mallinckrodt, and receives research funding from Bristol Myers Squibb. RAA receives research support from Bristol Myers Squibb and RAPT Therapeutics, and serves on advisory boards or consults for AstraZeneca, Bristol Myers Squibb, and Merck SD. EJL is an advisor/consultant for Bristol Myers Squibb, CareDX, Eisai, Genentech, HUYA Bioscience International, Immunocore, Instil Bio, Merck, Natera, Nektar, Novartis, Oncosec, Pfizer, Rain Therapeutics, Regeneron, Replimune, and Sanofi, and has research funding from Bristol Myers Squibb, Haystack Oncology, Merck, Regeneron, and Sanofi. DMP and SLT receive consulting fees from Amgen, Bristol Myers Squibb, Compugen, Dragonfly Therapeutics, Janssen Pharmaceuticals, Normunity, PathAI, RAPT Therapeutics, Regeneron, Takeda Pharmaceuticals, and Tizona LLC; receive research grants from Bristol Myers Squibb, Compugen, and Immunomic Therapeutics; have stock options or stock in Atengen Inc., DNAtrix, Dracen, Dragonfly Therapeutics, ManaT Bio, RAPT Therapeutics, and Tizona LLC; and have patents related to T-cell regulatory molecules including LAG-3, and the treatment of MSI-high cancers with anti-PD-1. JMT reports research grants and consulting fees from Akoya Biosciences and Bristol Myers Squibb; consulting for AstraZeneca, Compugen, Genentech, GlaxoSmithKline, Lunaphore, Merck, Regeneron and Roche; and an institutional patent filed on machine learning for scoring pathologic response to immunotherapy. TLM, AS, FS, J-WS, LAC-R, IRM, PS, AEB, JSD, QCZ, and JEH declare no potential conflicts of interest.
Figures


References
-
- Kawakami Y, Eliyahu S, Delgado CH, Robbins PF, Sakaguchi K, Appella E, et al. Identification of a human melanoma antigen recognized by tumor-infiltrating lymphocytes associated with in vivo tumor rejection. Proc Natl Acad Sci USA. 1994;91(14):6458–6462. doi: 10.1073/pnas.91.14.6458. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
