

The Story of Ammonia in Liver Disease: An Unraveling Continuum
- PMID: 38444405
- PMCID: PMC10910335
- DOI: 10.1016/j.jceh.2024.101361
The Story of Ammonia in Liver Disease: An Unraveling Continuum
Abstract
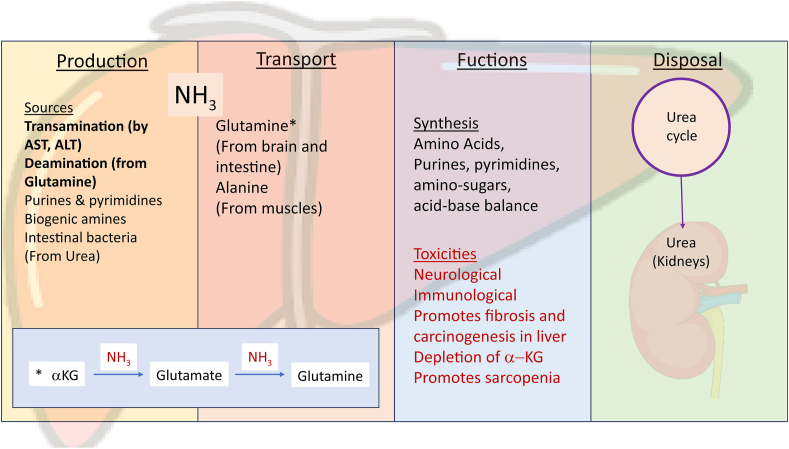
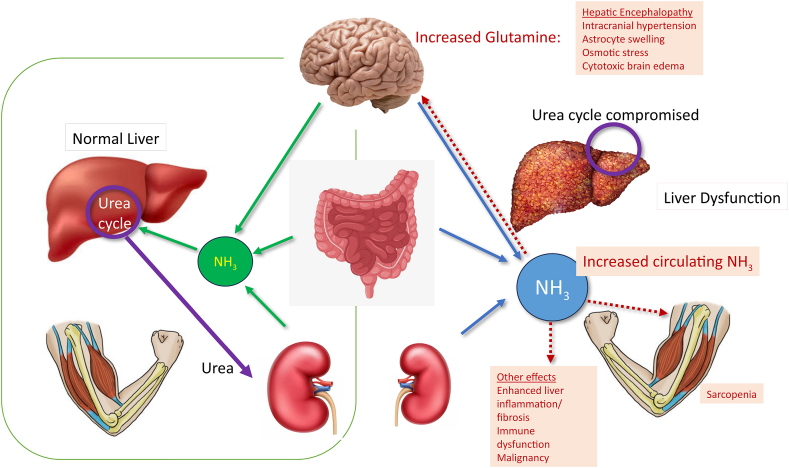
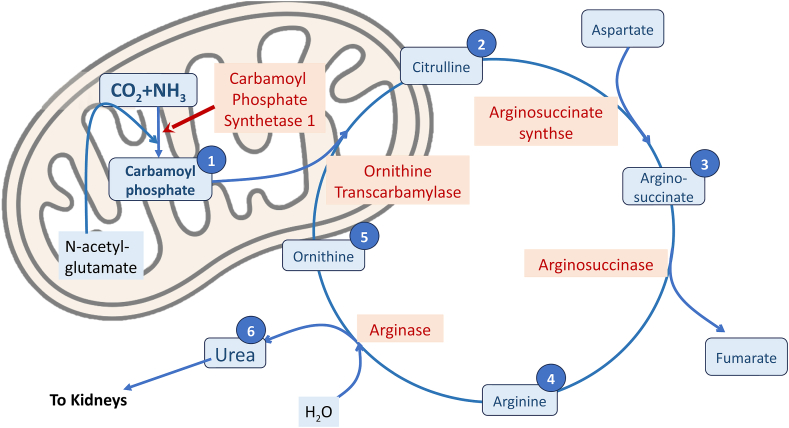
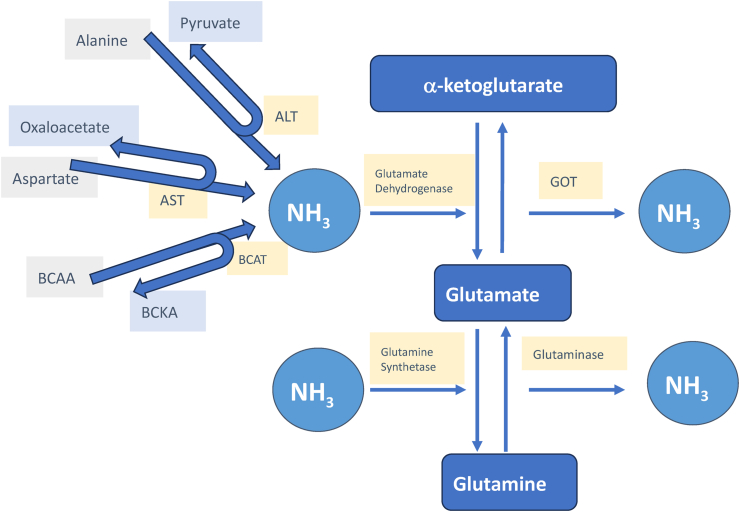
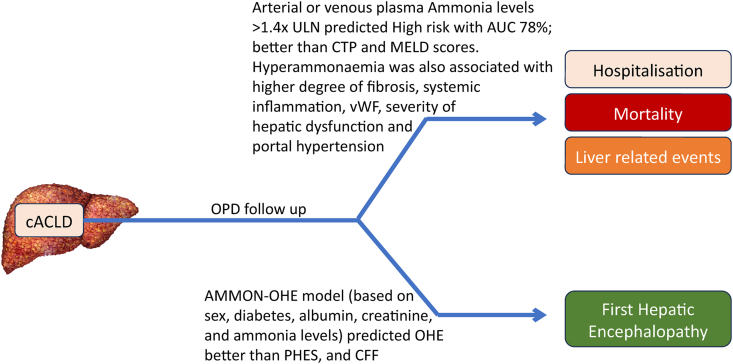
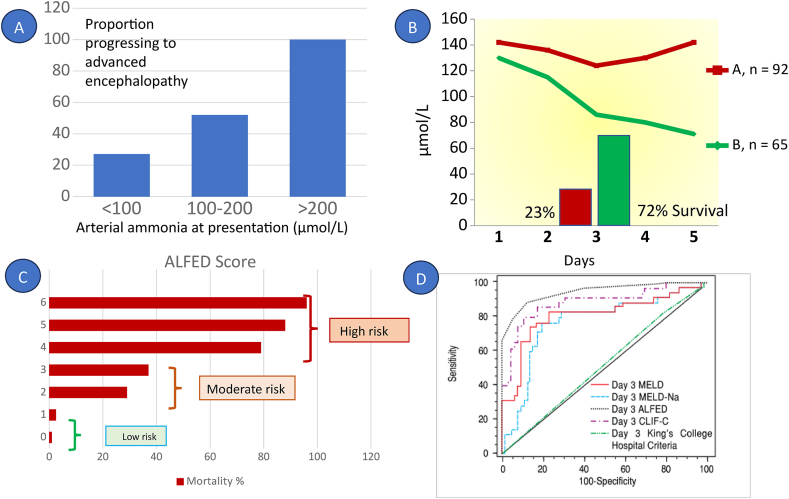
Hyperammonemia and liver disease are closely linked. Most of the ammonia in our body is produced by transamination and deamination activities involving amino acid, purine, pyrimidines, and biogenic amines, and from the intestine by bacterial splitting of urea. The only way of excretion from the body is by hepatic conversion of ammonia to urea. Hyperammonemia is associated with widespread toxicities such as cerebral edema, hepatic encephalopathy, immune dysfunction, promoting fibrosis, and carcinogenesis. Over the past two decades, it has been increasingly utilized for prognostication of cirrhosis, acute liver failure as well as acute on chronic liver failure. The laboratory assessment of hyperammonemia has certain limitations, despite which its value in the assessment of various forms of liver disease cannot be negated. It may soon become an important tool to make therapeutic decisions about the use of prophylactic and definitive treatment in various forms of liver disease.
Keywords: HE (hepatic encephalopathy); MASLD (metabolic dysfunction-associated steatotic liver disease); acute liver failure; ammonia; cACLD (compensated advanced chronic liver disease).
© 2024 Indian National Association for Study of the Liver. Published by Elsevier B.V.
Figures
Similar articles
-
Metabolic dysfunction-associated steatotic liver disease: A story of muscle and mass.World J Gastroenterol. 2025 May 28;31(20):105346. doi: 10.3748/wjg.v31.i20.105346. World J Gastroenterol. 2025. PMID: 40495947 Free PMC article.
-
NIH Consensus Statement on Management of Hepatitis C: 2002.NIH Consens State Sci Statements. 2002 Jun 10-12;19(3):1-46. NIH Consens State Sci Statements. 2002. PMID: 14768714
-
Rifaximin for prevention and treatment of hepatic encephalopathy in people with cirrhosis.Cochrane Database Syst Rev. 2023 Jul 19;7(7):CD011585. doi: 10.1002/14651858.CD011585.pub2. Cochrane Database Syst Rev. 2023. PMID: 37467180 Free PMC article.
-
The Midlands Liver Research Alliance - A partnership to optimise obesity-related liver disease research: targeting areas of high incidence and underserved communities.NIHR Open Res. 2024 Dec 12;4:75. doi: 10.3310/nihropenres.13784.1. eCollection 2024. NIHR Open Res. 2024. PMID: 40547821 Free PMC article.
-
X-Linked Protoporphyria.2013 Feb 14 [updated 2019 Nov 27]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 2013 Feb 14 [updated 2019 Nov 27]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 23409301 Free Books & Documents. Review.
Cited by
-
Metabolic Crosstalk between Liver and Brain: From Diseases to Mechanisms.Int J Mol Sci. 2024 Jul 11;25(14):7621. doi: 10.3390/ijms25147621. Int J Mol Sci. 2024. PMID: 39062868 Free PMC article. Review.
-
Enhancing Tetrahydrocannabinol's Therapeutic Efficacy in Inflammatory Bowel Disease: The Roles of Cannabidiol and the Cannabinoid 1 Receptor Allosteric Modulator ZCZ011.Pharmaceuticals (Basel). 2025 Jan 23;18(2):148. doi: 10.3390/ph18020148. Pharmaceuticals (Basel). 2025. PMID: 40005963 Free PMC article.
-
Improvement of Physical Functions in Elderly Patients with Heart Failure Depends on the Hepatic Reserve.Phys Ther Res. 2025;28(1):45-53. doi: 10.1298/ptr.E10328. Epub 2025 Mar 10. Phys Ther Res. 2025. PMID: 40321685 Free PMC article.
-
Gut‑liver axis in liver disease: From basic science to clinical treatment (Review).Mol Med Rep. 2025 Jan;31(1):10. doi: 10.3892/mmr.2024.13375. Epub 2024 Oct 25. Mol Med Rep. 2025. PMID: 39450549 Free PMC article. Review.
-
Comprehensive Assessment of Cannabidiol and HU308 in Acute and Chronic Colitis Models: Efficacy, Safety, and Mechanistic Innovations.Cells. 2024 Dec 5;13(23):2013. doi: 10.3390/cells13232013. Cells. 2024. PMID: 39682761 Free PMC article.
References
-
- Hahn M., Massen O., Nencki M., Pavlov I. Die Eck’sche fistel zwischen der unteren hohlvene und der pfortader und ihre folgen Fur den organismus. Arch. Exp. Pathol. 1893;32:161–210. Pharm. (Quoted by 1 ibid)
-
- Lockwood A., Yap E., Wong W. Cerebral ammonia metabolism in patients with severe liver disease and minimal hepatic encephalopathy. J Cerebr Blood Flow Metabol. 1991;11:337–341. - PubMed
-
- Mohiuddin S.S., Khattar D. StatPearls Publishing; 2023 Jan. Biochemistry, Ammonia.https://www.ncbi.nlm.nih.gov/books/NBK541039/ [Updated 2023 Feb 20]. In: StatPearls [Internet]. Treasure Island (FL) - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
