

Evaluating the impact of interprofessional training wards on patient satisfaction and clinical outcomes: a mixed-methods analysis
- PMID: 38444410
- PMCID: PMC10912604
- DOI: 10.3389/fmed.2024.1320027
Evaluating the impact of interprofessional training wards on patient satisfaction and clinical outcomes: a mixed-methods analysis
Abstract
Introduction: Interprofessional teamwork is pivotal in modern healthcare, prompting the establishment of interprofessional training wards since 1996. While these wards serve as hubs for optimizing healthcare professional collaboration and communication, research into patient outcomes remains notably sparse and geographically limited, predominantly examining patient satisfaction and sparingly exploring other metrics like mortality or self-discharge rates. This study seeks to bridge this gap, comparing patient outcomes in interprofessional training wards and conventional wards under the hypothesis that the former offers no disadvantage to patient outcomes.
Materials and methods: We explored patient outcomes within an interprofessional student ward called A-STAR at a University Hospital from October 2019 to December 2022. Engaging with patients discharged between May 2021 and April 2022, we utilized digital and paper-based anonymous questionnaires, catering to patient preference, to gather pertinent data.
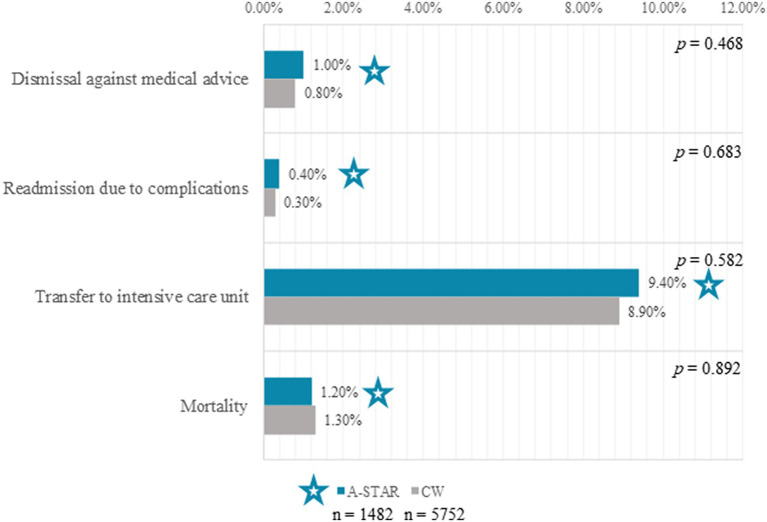
Results: Analysis of outcomes for 1,482 A-STAR (interprofessional student ward) and 5,752 conventional ward patients revealed noteworthy findings. A-STAR patients tended to be younger (59 vs. 61 years, p < 0.01) and more frequently male (73.5% vs. 70.4%, p = 0.025). Vital clinical outcomes, such as discharges against medical advice, complication-driven readmissions, and ICU transfers, were statistically similar between groups, as were mortality rates (1.2% vs. 1.3%, p = 0.468). A-STAR demonstrated high patient satisfaction, underscored by positive reflections on team competence, ward atmosphere, and responsiveness to concerns, emphasizing the value placed on interprofessional collaboration. Patient narratives commended team kindness, lucid explanations, and proactive involvement.
Discussion: This data collectively underscores the safety and reliability of patient care within training wards, affirming that patients can trust the care provided in these settings. Patients on the interprofessional ward demonstrated high satisfaction levels: 96.7% appreciated the atmosphere and conduct of ward rounds. In comparison, 98.3% were satisfied with the discussion and information about their treatment during their hospital stay.
Keywords: clinical outcome; collaborative care; healthcare education; internal medicine; interprofessional education; interprofessional training ward; patient satisfaction; quality of care.
Copyright © 2024 Schlosser-Hupf, Aichner, Meier, Albaladejo-Fuertes, Ruttmann, Rusch, Michels, Mehrl, Kunst, Schmid and Müller.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




Similar articles
-
Cost-effectiveness in an interprofessional training ward within a university department for internal medicine: a monocentric open-label controlled study of the A-STAR Regensburg.Front Public Health. 2024 Aug 9;12:1340953. doi: 10.3389/fpubh.2024.1340953. eCollection 2024. Front Public Health. 2024. PMID: 39185108 Free PMC article.
-
Development of individual competencies and team performance in interprofessional ward rounds: results of a study with multimodal observations at the Heidelberg Interprofessional Training Ward.Front Med (Lausanne). 2023 Sep 27;10:1241557. doi: 10.3389/fmed.2023.1241557. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37828945 Free PMC article.
-
The impact of an interprofessional training ward on the development of interprofessional competencies: study protocol of a longitudinal mixed-methods study.BMC Med Educ. 2019 Feb 7;19(1):48. doi: 10.1186/s12909-019-1478-1. BMC Med Educ. 2019. PMID: 30732614 Free PMC article.
-
A review of interprofessional training wards: Enhancing student learning and patient outcomes.Med Teach. 2019 May;41(5):547-554. doi: 10.1080/0142159X.2018.1503410. Epub 2018 Nov 3. Med Teach. 2019. PMID: 30394168 Review.
-
Call the On-Call: a study of student learning on an interprofessional training ward.J Interprof Care. 2021 Mar-Apr;35(2):275-283. doi: 10.1080/13561820.2020.1725452. Epub 2020 Feb 27. J Interprof Care. 2021. PMID: 32105153 Review.
Cited by
-
Interprofessional Therapeutic Drug Monitoring of Piperacillin/Tazobactam Enhances Care for Patients with Acute-on-Chronic Liver Failure in the ICU: A Retrospective Observational Pilot Study.Antibiotics (Basel). 2025 Feb 14;14(2):202. doi: 10.3390/antibiotics14020202. Antibiotics (Basel). 2025. PMID: 40001445 Free PMC article.
-
Cost-effectiveness in an interprofessional training ward within a university department for internal medicine: a monocentric open-label controlled study of the A-STAR Regensburg.Front Public Health. 2024 Aug 9;12:1340953. doi: 10.3389/fpubh.2024.1340953. eCollection 2024. Front Public Health. 2024. PMID: 39185108 Free PMC article.
References
-
- Gilbert JH, Yan J, Hoffman SJ. A WHO report: framework for action on interprofessional education and collaborative practice. J Allied Health. (2010) 1:196–7., PMID: - PubMed
-
- Villalobos M, Deis N, Wesselmann S, Seufferlein T, Ehlers F, Mahler C, et al. . Heidelberger Meilenstein Kommunikation (HeiMeKOM) – Erfahrungen, Best Practice Beispiele und Empfehlungen aus dem Abschluss-Symposium am 30./31. Januar 2020. Gesundheitswesen. (2022) 84:968–70. doi: 10.1055/a-1375-0922, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous