

Retrospective cohort study investigating association between precancerous gastric lesions and colorectal neoplasm risk
- PMID: 38444677
- PMCID: PMC10914248
- DOI: 10.3389/fonc.2024.1320020
Retrospective cohort study investigating association between precancerous gastric lesions and colorectal neoplasm risk
Abstract
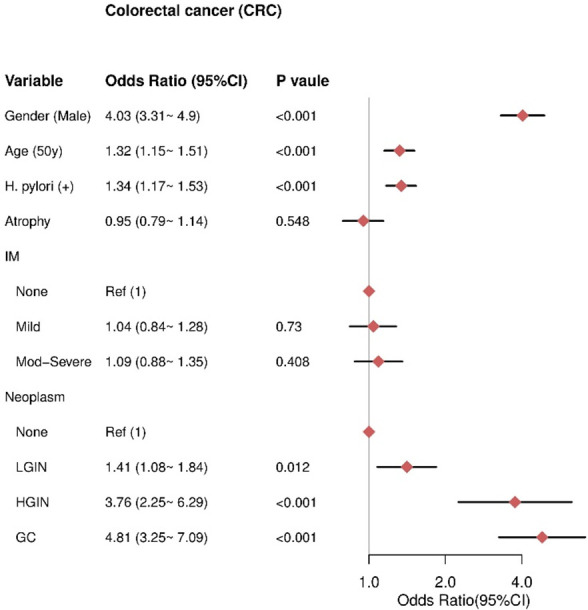
Background: Colorectal cancer (CRC) is considered the most prevalent synchronous malignancy in patients with gastric cancer. This large retrospective study aims to clarify correlations between gastric histopathology stages and risks of specific colorectal neoplasms, to optimize screening and reduce preventable CRC.
Methods: Clinical data of 36,708 patients undergoing gastroscopy and colonoscopy from 2005-2022 were retrospectively analyzed. Correlations between gastric and colorectal histopathology were assessed by multivariate analysis. Outcomes of interest included non-adenomatous polyps (NAP), conventional adenomas (CAs), serrated polyps (SPs), and CRC. Statistical analysis used R version 4.0.4.
Results: Older age (≥50 years) and Helicobacter pylori infection (HPI) were associated with increased risks of conventional adenomas (CAs), serrated polyps (SPs), non-adenomatous polyps (NAP), and colorectal cancer (CRC). Moderate to severe intestinal metaplasia specifically increased risks of NAP and CAs by 1.17-fold (95% CI 1.05-1.3) and 1.19-fold (95% CI 1.09-1.31), respectively. For CRC risk, low-grade intraepithelial neoplasia increased risk by 1.41-fold (95% CI 1.08-1.84), while high-grade intraepithelial neoplasia (OR 3.76, 95% CI 2.25-6.29) and gastric cancer (OR 4.81, 95% CI 3.25-7.09) showed strong associations. More advanced gastric pathology was correlated with progressively higher risks of CRC.
Conclusion: Precancerous gastric conditions are associated with increased colorectal neoplasm risk. Our findings can inform screening guidelines to target high-risk subgroups, advancing colorectal cancer prevention and reducing disease burden.
Keywords: atrophic gastritis; colorectal adenoma; helicobacter pylori; intestinal metaplasia; serrated lesions.
Copyright © 2024 Pan, Zhang, Fang, Chen, He, Zheng and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




Similar articles
-
The Potential Value of Gastric Histopathology for Predicting Colorectal Adenomatous Polyps Among the Chinese Population: A Retrospective Cross-Sectional Study.Front Oncol. 2022 Jul 6;12:889417. doi: 10.3389/fonc.2022.889417. eCollection 2022. Front Oncol. 2022. PMID: 35875116 Free PMC article.
-
Association of Helicobacter pylori infection with colorectal polyps and malignancy in China.World J Gastrointest Oncol. 2020 May 15;12(5):582-591. doi: 10.4251/wjgo.v12.i5.582. World J Gastrointest Oncol. 2020. PMID: 32461789 Free PMC article.
-
Esophagogastroscopic Abnormalities Potentially Guided Patients Younger than 50 Years Old to Undergo Colonoscopy Earlier: A Retrospective Cross-Sectional Study.Dig Dis Sci. 2024 Jan;69(1):36-44. doi: 10.1007/s10620-023-08158-y. Epub 2023 Nov 21. Dig Dis Sci. 2024. PMID: 37989896
-
Sessile Serrated Adenomas: How to Detect, Characterize and Resect.Gut Liver. 2017 Nov 15;11(6):747-760. doi: 10.5009/gnl16523. Gut Liver. 2017. PMID: 28494577 Free PMC article. Review.
-
Gastric atrophy, metaplasia, and dysplasia: a clinical perspective.J Clin Gastroenterol. 2003 May-Jun;36(5 Suppl):S29-36; discussion S61-2. doi: 10.1097/00004836-200305001-00006. J Clin Gastroenterol. 2003. PMID: 12702963 Review.
Cited by
-
Increased risk of colorectal cancer in young males with higher cardiovascular risk: A nationwide population-based cohort study.World J Gastrointest Oncol. 2025 Mar 15;17(3):101260. doi: 10.4251/wjgo.v17.i3.101260. World J Gastrointest Oncol. 2025. PMID: 40092948 Free PMC article.
-
Gastric Polyps Detected Incidentally during Gastroscopy and Follow-Up Results.J Clin Med. 2024 May 26;13(11):3117. doi: 10.3390/jcm13113117. J Clin Med. 2024. PMID: 38892828 Free PMC article.
-
Helicobacter pylori infection, anti-Helicobacter pylori treatment and risk of colorectal cancer and adenoma: an observational study and a meta-analysis.EClinicalMedicine. 2025 Jun 9;84:103299. doi: 10.1016/j.eclinm.2025.103299. eCollection 2025 Jun. EClinicalMedicine. 2025. PMID: 40547441 Free PMC article.
-
Helicobacter pylori Infection in Patients with Gastric Cancer: A 2024 Update.Cancers (Basel). 2024 May 22;16(11):1958. doi: 10.3390/cancers16111958. Cancers (Basel). 2024. PMID: 38893079 Free PMC article. Review.
References
-
- Sánchez Gómez CA, Tejido Sandoval C, de Vicente Bielza N, Pin Vieito N, González A, Almazán R, et al. . Surgical complications in a population-based colorectal cancer screening program: Incidence and associated factors. Gastroenterol Hepatol (2022) 45:660–7. doi: 10.1016/j.gastre.2022.03.001. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials