

Successful permanent pacemaker explantation after diagnosis and treatment of Lyme carditis complete heart block: a case report
- PMID: 38444881
- PMCID: PMC10914342
- DOI: 10.1093/ehjcr/ytad576
Successful permanent pacemaker explantation after diagnosis and treatment of Lyme carditis complete heart block: a case report
Abstract
Background: Lyme carditis (LC) complete heart block (CHB) is typically treated with i.v. antibiotics without requiring permanent pacing. In patients with high degree atrioventricular (AV) block, suspicious index in Lyme carditis (SILC) scoring is highly sensitive for diagnosing LC.
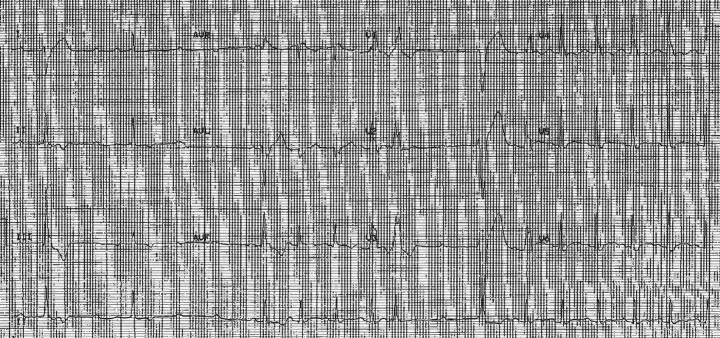
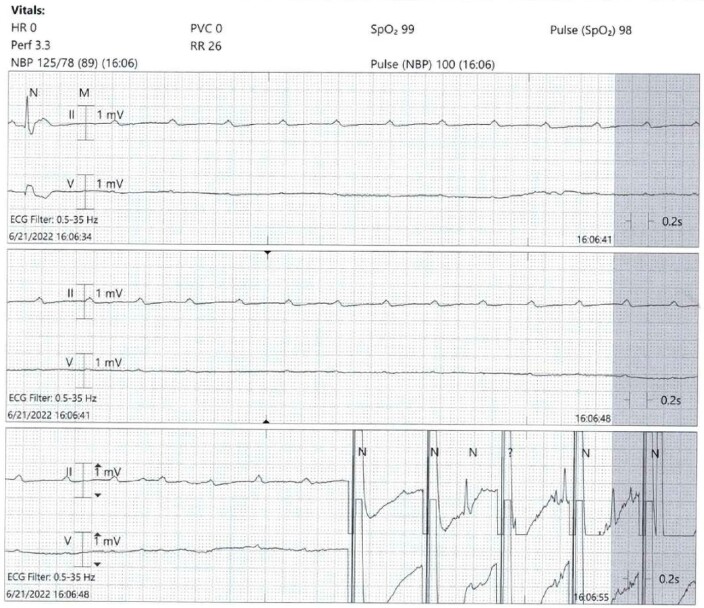
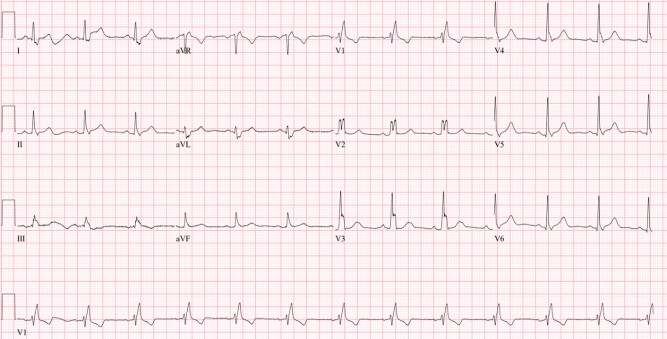
Case summary: We present a case of CHB where a permanent pacemaker (PPM) was implanted prior to LC diagnosis. Suspicious index in Lyme carditis score was 2 at the time of exam, indicating a low risk for LC. However, per further discussion at follow-up, his score was retroactively increased to an intermediate risk of 4 and Lyme titres returned positive. An outpatient oral antibiotic regimen was given, and 2 months later, the patient had <0.1% V-pacing on interrogation with a subsequent unremarkable event monitor. The pacemaker was removed after considerations ensuring full conduction recovery. The patient is doing well at follow-up > 1 year.
Discussion: Lyme carditis spontaneous resolution of CHB is common. Once safe extraction parameters have been established, it is appropriate to engage patients without ongoing pacer requirements about explantation of their PPM. For CHB patients without clear aetiology, SILC scoring may be a predictive measure to help prevent unnecessary PPM placement in the future.
Keywords: Arrhythmias; Case report; Complete heart block; Lyme carditis; Pacemaker.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
Similar articles
-
Pacemaker Explantation in Patients With Lyme Carditis.JACC Case Rep. 2022 May 18;4(10):613-616. doi: 10.1016/j.jaccas.2022.02.012. eCollection 2022 May 18. JACC Case Rep. 2022. PMID: 35615211 Free PMC article.
-
Early-onset Lyme carditis with concurrent disseminated erythema migrans.Am J Cardiovasc Dis. 2017 Apr 15;7(2):53-56. eCollection 2017. Am J Cardiovasc Dis. 2017. PMID: 28533930 Free PMC article.
-
Reversible atrioventricular block and the importance of close follow-up: Two cases of Lyme carditis.J Cardiol Cases. 2018 Feb 13;17(5):171-174. doi: 10.1016/j.jccase.2018.01.001. eCollection 2018 May. J Cardiol Cases. 2018. PMID: 30279884 Free PMC article.
-
Suspicious index in Lyme carditis: Systematic review and proposed new risk score.Clin Cardiol. 2018 Dec;41(12):1611-1616. doi: 10.1002/clc.23102. Epub 2018 Nov 26. Clin Cardiol. 2018. PMID: 30350436 Free PMC article.
-
The Value of the Surface ECG for the Diagnosis and Management of Lyme Carditis: A Case Report.Curr Cardiol Rev. 2021;17(1):5-9. doi: 10.2174/1573403X16666200312101751. Curr Cardiol Rev. 2021. PMID: 32164515 Free PMC article. Review.
References
-
- Lantos PM, Rumbaugh J, Bockenstedt LK, Falck-Ytter Y, Aguero-Rosenfeld M, Auwaerter P, et al. . Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 guidelines for the prevention, diagnosis and treatment of Lyme disease. Clin Infect Dis 2021;72:e1–e48. - PubMed
-
- Yeung C, Baranchuk A. Diagnosis and treatment of Lyme carditis. J Am Coll Cardiol 2019;73:717–726. - PubMed
-
- Fuster LS, Gul EE, Baranchuk A. Electrocardiographic progression of acute Lyme disease. Am J Emerg Med 2017;35:1040.e5–1040.e6. - PubMed
-
- Wan D, Blakely C, Branscombe P, Suarez-Fuster L, Glover B, Baranchuk A. Lyme carditis and high-degree atrioventricular block. Am J Cardiol. 2018;121:1102–1104. - PubMed
Publication types
LinkOut - more resources
Full Text Sources