

Longitudinal Rates of Change in Structural Parameters of Optical Coherence Tomography in Primary Angle Closure Glaucoma following Laser Iridotomy along with Peripheral Iridoplasty
- PMID: 38445101
- PMCID: PMC10914411
- DOI: 10.1155/2024/9978354
Longitudinal Rates of Change in Structural Parameters of Optical Coherence Tomography in Primary Angle Closure Glaucoma following Laser Iridotomy along with Peripheral Iridoplasty
Abstract
Background: This study aimed to investigate longitudinal rates of change (LRCs) of structural parameters from optical coherence tomography (OCT) in patients with primary angle closure glaucoma (PACG) after laser iridotomy (LI) along with laser peripheral iridoplasty (PI).
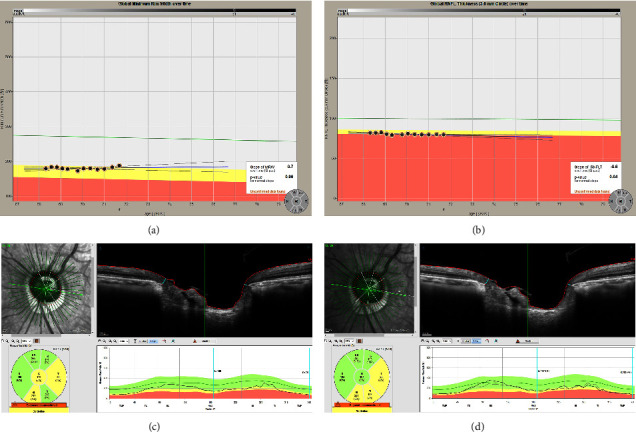
Methods: Among 146 patients diagnosed with PACG, thirty-two subjects (32 eyes) who underwent LI plus PI and accomplished more than five times of reliable OCT tests were included in the current retrospective study. Retinal nerve fiber layer (RNFL) and Bruch's membrane opening-minimum rim width (BMO-MRW) were measured by spectral-domain OCT with three month interval. LRCs of global and six Garway-Heath sectors were investigated using the linear mixed-effects model which adjusted BMO area, sex, and age. Imaging of dual Scheimpflug analyzer was performed before and at 1 week after LI with PI and yearly thereafter.
Results: The mean follow-up period was 32.28 ± 13.34 months with a mean number of 10.18 ± 3.33 OCT images. Baseline characteristics are as follows: age, 63 ± 7.9 years; female, 62.5%; intraocular pressure(IOP), 15.48 ± 4.79 mmHg; anterior chamber depth, 2.09 ± 0.18 mm; and mean deviation, -7.97 ± 8.48 dB. Global LRC of BMO-MRW was 0.86 ± 1.34 μm/yr and RNFL was -0.64 ± 0.22 μm/yr. IOP decreased significantly to 13.06 ± 2.21 mmHg (p=0.001) while anterior chamber volume (p=0.011) and mean anterior chamber angle (p=0.022) increased significantly after LI along with PI compared to the baseline at the final visit.
Conclusions: LRC of a new parameter, BMO-MRW, and LRC of RNFL were relatively low in patients with PACG, following LI along with PI. After widening of the anterior chamber angle and decrease of IOP due to LI plus PI, PACG might show stable structural prognosis assessed by OCT.
Copyright © 2024 Hyun-Kyung Cho and Changwon Kee.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Rate of Change in Bruch's Membrane Opening-Minimum Rim Width and Peripapillary RNFL in Early Normal Tension Glaucoma.J Clin Med. 2020 Jul 22;9(8):2321. doi: 10.3390/jcm9082321. J Clin Med. 2020. PMID: 32707745 Free PMC article.
-
Comparison of Rate of Change between Bruch's Membrane Opening Minimum Rim Width and Retinal Nerve Fiber Layer in Eyes Showing Optic Disc Hemorrhage.Am J Ophthalmol. 2020 Sep;217:27-37. doi: 10.1016/j.ajo.2020.03.051. Epub 2020 Apr 10. Am J Ophthalmol. 2020. PMID: 32283093
-
Laser peripheral iridoplasty for chronic angle closure.Cochrane Database Syst Rev. 2021 Mar 23;3(3):CD006746. doi: 10.1002/14651858.CD006746.pub4. Cochrane Database Syst Rev. 2021. PMID: 33755197 Free PMC article.
-
Novel Bruch's Membrane Opening Minimum Rim Area Equalizes Disc Size Dependency and Offers High Diagnostic Power for Glaucoma.Invest Ophthalmol Vis Sci. 2016 Dec 1;57(15):6596-6603. doi: 10.1167/iovs.16-20561. Invest Ophthalmol Vis Sci. 2016. PMID: 27951592
-
Anterior Segment Optical Coherence Tomography Changes to the Anterior Chamber Angle in the Short-term following Laser Peripheral Iridoplasty.J Curr Glaucoma Pract. 2014 Jan-Apr;8(1):1-6. doi: 10.5005/jp-journals-10008-1152. Epub 2014 Jan 16. J Curr Glaucoma Pract. 2014. PMID: 26997799 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
