

Dyslipidemia in American Indian Adolescents and Young Adults: Strong Heart Family Study
- PMID: 38445515
- PMCID: PMC11010025
- DOI: 10.1161/JAHA.123.031741
Dyslipidemia in American Indian Adolescents and Young Adults: Strong Heart Family Study
Abstract
Background: Although many studies on the association between dyslipidemia and cardiovascular disease (CVD) exist in older adults, data on the association among adolescents and young adults living with disproportionate burden of cardiometabolic disorders are scarce.
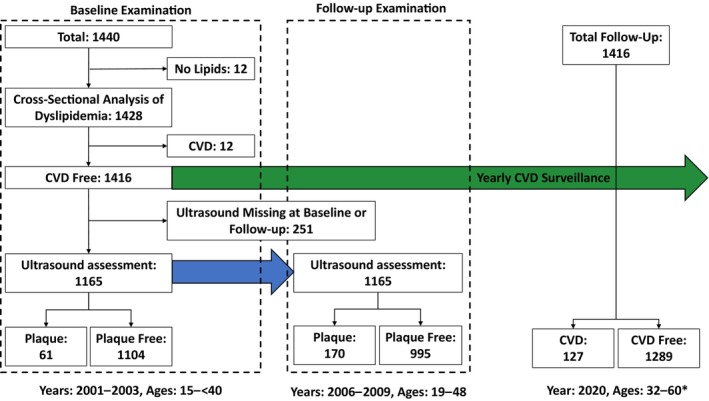
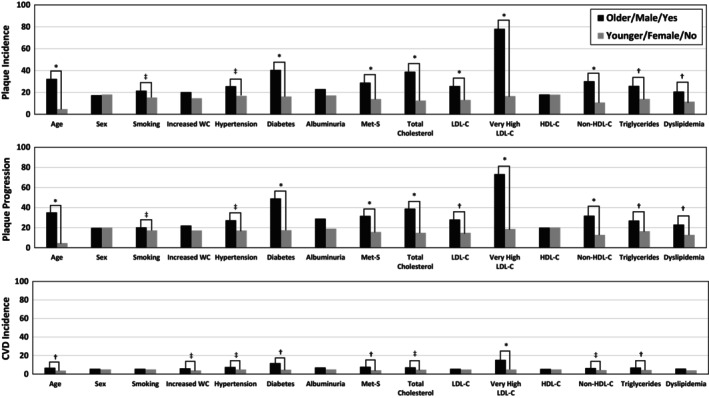
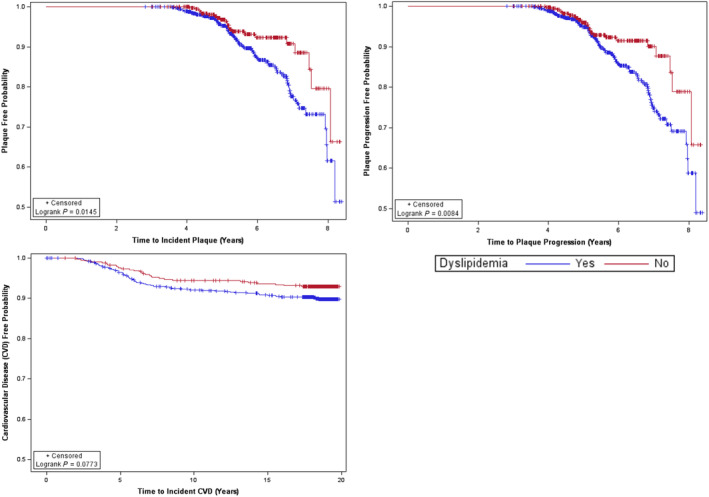
Methods and results: The SHFS (Strong Heart Family Study) is a multicenter, family-based, prospective cohort study of CVD in an American Indian populations, including 12 communities in central Arizona, southwestern Oklahoma, and the Dakotas. We evaluated SHFS participants, who were 15 to 39 years old at the baseline examination in 2001 to 2003 (n=1440). Lipids were measured after a 12-hour fast. We used carotid ultrasounds to detect plaque at baseline and follow-up in 2006 to 2009 (median follow-up=5.5 years). We identified incident CVD events through 2020 with a median follow-up of 18.5 years. We used shared frailty proportional hazards models to assess the association between dyslipidemia and subclinical or clinical CVD, while controlling for covariates. Baseline dyslipidemia prevalence was 55.2%, 73.6%, and 78.0% for participants 15 to 19, 20 to 29, and 30 to 39 years old, respectively. Approximately 2.8% had low-density lipoprotein cholesterol ≥160 mg/dL, which is higher than the recommended threshold for lifestyle or medical interventions in young adults of 20 to 39 years old. During follow-up, 9.9% had incident plaque (109/1104 plaque-free participants with baseline and follow-up ultrasounds), 11.0% had plaque progression (128/1165 with both baseline and follow-up ultrasounds), and 9% had incident CVD (127/1416 CVD-free participants at baseline). Plaque incidence and progression were higher in participants with total cholesterol ≥200 mg/dL, low-density lipoprotein cholesterol ≥160 mg/dL, or non-high-density lipoprotein cholesterol ≥130 mg/dL, while controlling for covariates. CVD risk was independently associated with low-density lipoprotein cholesterol ≥160 mg/dL.
Conclusions: Dyslipidemia is a modifiable risk factor that is associated with both subclinical and clinical CVD, even among the younger American Indian population who have unexpectedly high rates of significant CVD events. Therefore, this population is likely to benefit from a variety of evidence-based interventions including screening, educational, lifestyle, and guideline-directed medical therapy at an early age.
Keywords: American Indian; Strong Heart Family Study; adolescent; atherosclerosis; cardiovascular disease; dyslipidemia; young adult.
Figures
Similar articles
-
Subclinical atherosclerosis in adolescents and young adults and the risk of cardiovascular disease: The Strong Heart Family Study (SHFS).Nutr Metab Cardiovasc Dis. 2022 Aug;32(8):1863-1871. doi: 10.1016/j.numecd.2022.04.024. Epub 2022 May 10. Nutr Metab Cardiovasc Dis. 2022. PMID: 35680485 Free PMC article.
-
Utility of 2013 American College of Cardiology/American Heart Association Cholesterol Guidelines in HIV-Infected Adults With Carotid Atherosclerosis.Circ Cardiovasc Imaging. 2017 Jul;10(7):e005995. doi: 10.1161/CIRCIMAGING.116.005995. Circ Cardiovasc Imaging. 2017. PMID: 28674084 Free PMC article.
-
Childhood Dyslipidemia and Carotid Atherosclerotic Plaque in Adulthood: The Cardiovascular Risk in Young Finns Study.J Am Heart Assoc. 2023 Apr 4;12(7):e027586. doi: 10.1161/JAHA.122.027586. Epub 2023 Mar 16. J Am Heart Assoc. 2023. PMID: 36927037 Free PMC article.
-
Lowering Targeted Atherogenic Lipoprotein Cholesterol Goals for Patients at "Extreme" ASCVD Risk.Curr Diab Rep. 2019 Nov 21;19(12):146. doi: 10.1007/s11892-019-1246-y. Curr Diab Rep. 2019. PMID: 31754844 Review.
-
Primary prevention of coronary heart disease: integration of new data, evolving views, revised goals, and role of rosuvastatin in management. A comprehensive survey.Drug Des Devel Ther. 2011;5:325-80. doi: 10.2147/DDDT.S14934. Epub 2011 Jun 13. Drug Des Devel Ther. 2011. PMID: 21792295 Free PMC article. Review.
Cited by
-
Obesity and Left Ventricular Function in American Indian Adolescents: Strong Heart Family Study.J Racial Ethn Health Disparities. 2024 Oct 18. doi: 10.1007/s40615-024-02216-5. Online ahead of print. J Racial Ethn Health Disparities. 2024. PMID: 39422831
-
Longitudinal Lipidomic Profile of Subclinical Peripheral Artery Disease in American Indians: The Strong Heart Family Study.Prev Chronic Dis. 2025 May 8;22:E18. doi: 10.5888/pcd22.240220. Prev Chronic Dis. 2025. PMID: 40338792 Free PMC article.
-
Vitamin D Deficiency and Cardiovascular Disease Risk Factors Among American Indian Adolescents: The Strong Heart Family Study.Prev Chronic Dis. 2025 Apr 3;22:E13. doi: 10.5888/pcd22.240354. Prev Chronic Dis. 2025. PMID: 40179031 Free PMC article.
-
Intersectionality and Social Drivers of Health in Cardiovascular Care.Methodist Debakey Cardiovasc J. 2024 Nov 5;20(5):98-110. doi: 10.14797/mdcvj.1436. eCollection 2024. Methodist Debakey Cardiovasc J. 2024. PMID: 39525384 Free PMC article. Review.
-
Cardiovascular Disease Risk Factors in the Native American Population.J Cardiovasc Dev Dis. 2025 Jan 16;12(1):27. doi: 10.3390/jcdd12010027. J Cardiovasc Dev Dis. 2025. PMID: 39852305 Free PMC article. Review.
References
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, Delling FN, et al. Heart disease and stroke statistics‐2021 update: a report from the American Heart Association. Circulation. 2021;143:e254–e743. doi: 10.1161/cir.0000000000000950 - DOI - PubMed
-
- Xu J, Lee ET, Peterson LE, Devereux RB, Rhoades ER, Umans JG, Best LG, Howard WJ, Paranilam J, Howard BV. Differences in risk factors for coronary heart disease among diabetic and nondiabetic individuals from a population with high rates of diabetes: the Strong Heart Study. J Clin Endocrinol Metab. 2012;97:3766–3774. doi: 10.1210/jc.2012-2110 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
