

The role of T-type calcium channels in elderly human vascular function: A pilot randomized controlled trial
- PMID: 38445814
- PMCID: PMC11061624
- DOI: 10.1113/EP091645
The role of T-type calcium channels in elderly human vascular function: A pilot randomized controlled trial
Abstract
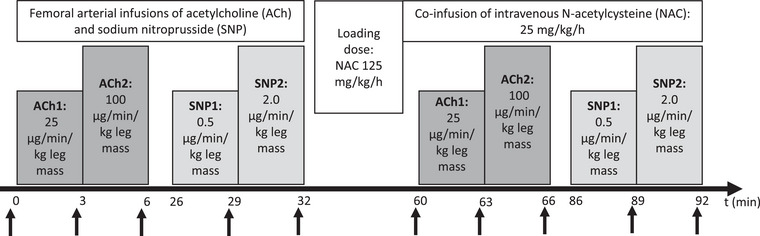
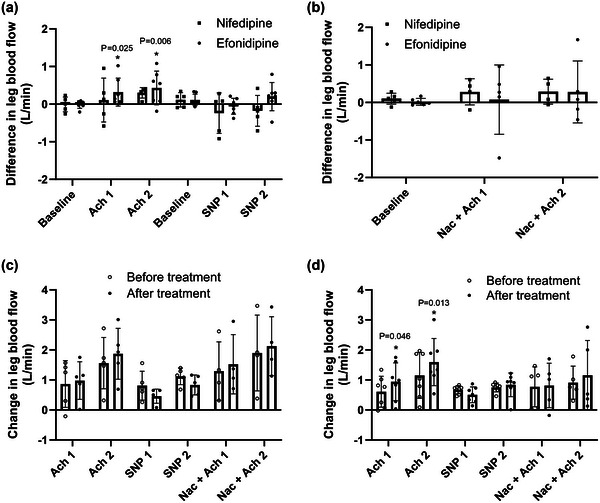
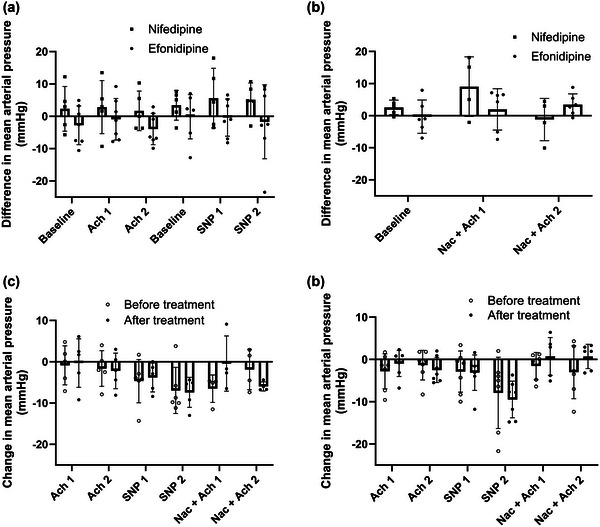
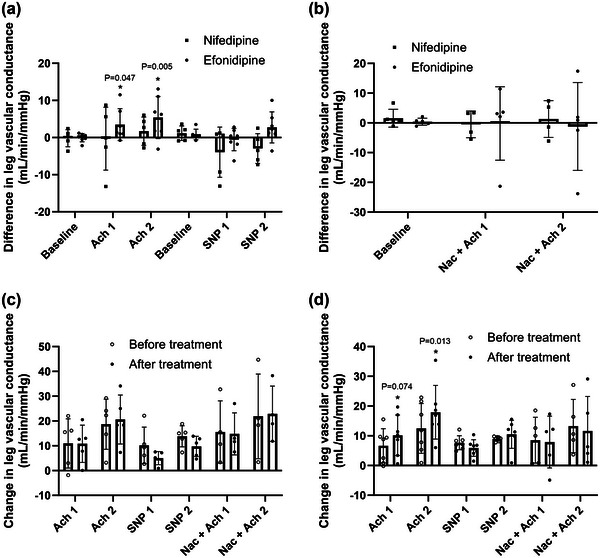
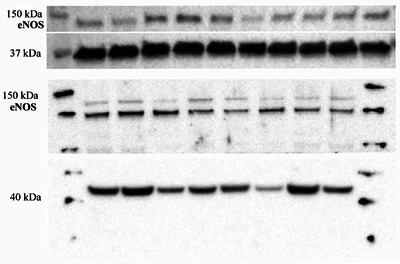
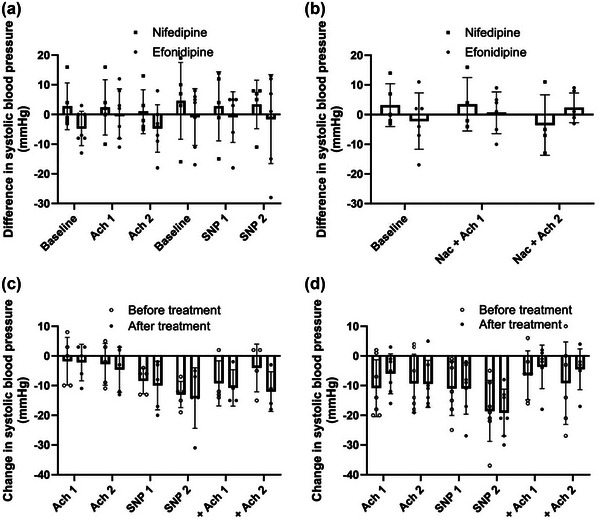
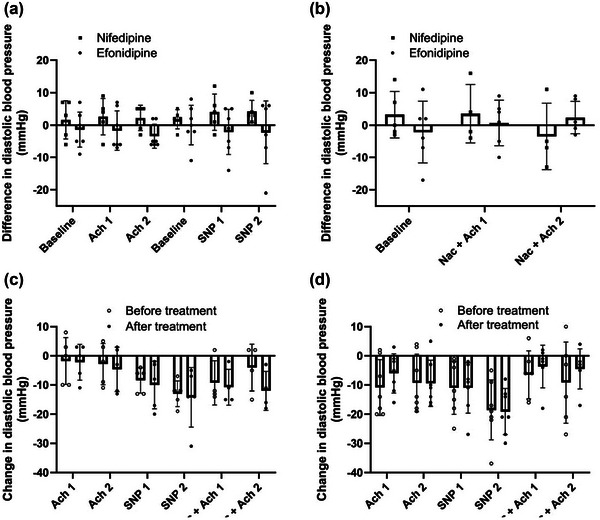
Endothelial dysfunction develops with age and may precede cardiovascular disease. Animal data suggest that T-type calcium channels play an important role in endothelial function, but data from humans are lacking. This study included 15 healthy, sedentary, elderly males for a double blinded, randomized controlled trial. For 8 weeks, they were given 40 mg/day of either efonidipine (L- and T-type calcium channel blocker (CCB)) or nifedipine (L-type CCB). Vascular function was evaluated by graded femoral arterial infusions of acetylcholine (ACh; endothelium-dependent vasodilator) and sodium nitroprusside (endothelium-independent vasodilator) both with and without co-infusion of N-acetylcysteine (NAC; antioxidant). We measured leg blood flow and mean arterial pressure and calculated leg vascular conductance to evaluate the leg vascular responses. Despite no significant change in blood pressure in either group, we observed higher leg blood flow responses (Δ 0.43 ± 0.45 l/min, P = 0.006) and leg vascular conductance (Δ 5.38 ± 5.67 ml/min/mmHg, P = 0.005) to intra-arterial ACh after efonidipine, whereas there was no change in the nifedipine group, and no differences between groups. We found no upregulation of endothelial nitric oxide synthase in vastus lateralis muscle biopsies within or between groups. Smooth muscle cell responsiveness was unaltered by efonidipine or nifedipine. Intravenous co-infusion of NAC did not affect endothelium-dependent vasodilatation in either of the CCB groups. These results suggest that 8 weeks' inhibition of T- and L-type calcium channels augments endothelium-dependent vasodilatory function in healthy elderly males. Further studies are required to elucidate if T-type calcium channel inhibition can counteract endothelial dysfunction.
Keywords: acetylcholine receptor; blood vessels; cardiovascular; endothelium; hypertension.
© 2024 The Authors. Experimental Physiology published by John Wiley & Sons Ltd on behalf of The Physiological Society.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- Celermajer, D. S. , Sorensen, K. E. , Spiegelhalter, D. J. , Georgakopoulos, D. , Robinson, J. , & Deanfield, J. E. (1994a). Aging is associated with endothelial dysfunction in healthy men years before the age‐related decline in women. Journal of the American College of Cardiology, 24(2), 471–476. - PubMed
-
- Celermajer, D. S. , Sorensen, K. E. , Spiegelhalter, D. J. , Georgakopoulos, D. , Robinson, J. , & Deanfield, J. E. (1994b). Aging is associated with endothelial dysfunction in healthy men years before the age‐related decline in women. Journal of the American College of Cardiology, 24(2), 471–476. - PubMed
-
- Clifford, P. S. , & Hellsten, Y. (2004). Vasodilatory mechanisms in contracting skeletal muscle. Journal of Applied Physiology, 97(1), 393–403. - PubMed
-
- Delaney, E. P. , Greaney, J. L. , Edwards, D. G. , Rose, W. C. , Fadel, P. J. , & Farquhar, W. B. (2010). Exaggerated sympathetic and pressor responses to handgrip exercise in older hypertensive humans: Role of the muscle metaboreflex. American Journal of Physiology‐Heart and Circulatory Physiology, 299(5), H1318–H1327. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources