

Implantable loop recorders in patients with Brugada syndrome: the BruLoop study
- PMID: 38445836
- PMCID: PMC10998731
- DOI: 10.1093/eurheartj/ehae133
Implantable loop recorders in patients with Brugada syndrome: the BruLoop study
Erratum in
-
Correction to: Implantable loop recorders in patients with Brugada syndrome: the BruLoop study.Eur Heart J. 2024 Jun 14;45(23):2104. doi: 10.1093/eurheartj/ehae273. Eur Heart J. 2024. PMID: 38722639 Free PMC article. No abstract available.
Abstract
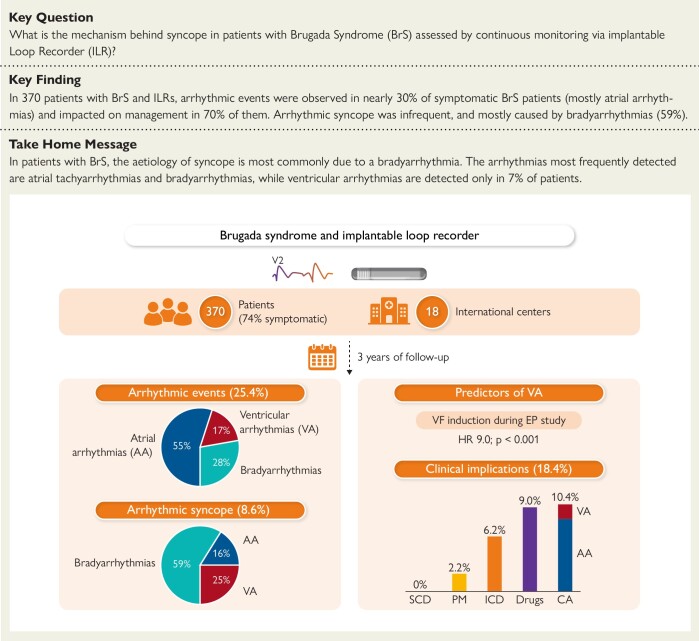
Background and aims: Available data on continuous rhythm monitoring by implantable loop recorders (ILRs) in patients with Brugada syndrome (BrS) are scarce. The aim of this multi-centre study was to evaluate the diagnostic yield and clinical implication of a continuous rhythm monitoring strategy by ILRs in a large cohort of BrS patients and to assess the precise arrhythmic cause of syncopal episodes.
Methods: A total of 370 patients with BrS and ILRs (mean age 43.5 ± 15.9, 33.8% female, 74.1% symptomatic) from 18 international centers were included. Patients were followed with continuous rhythm monitoring for a median follow-up of 3 years.
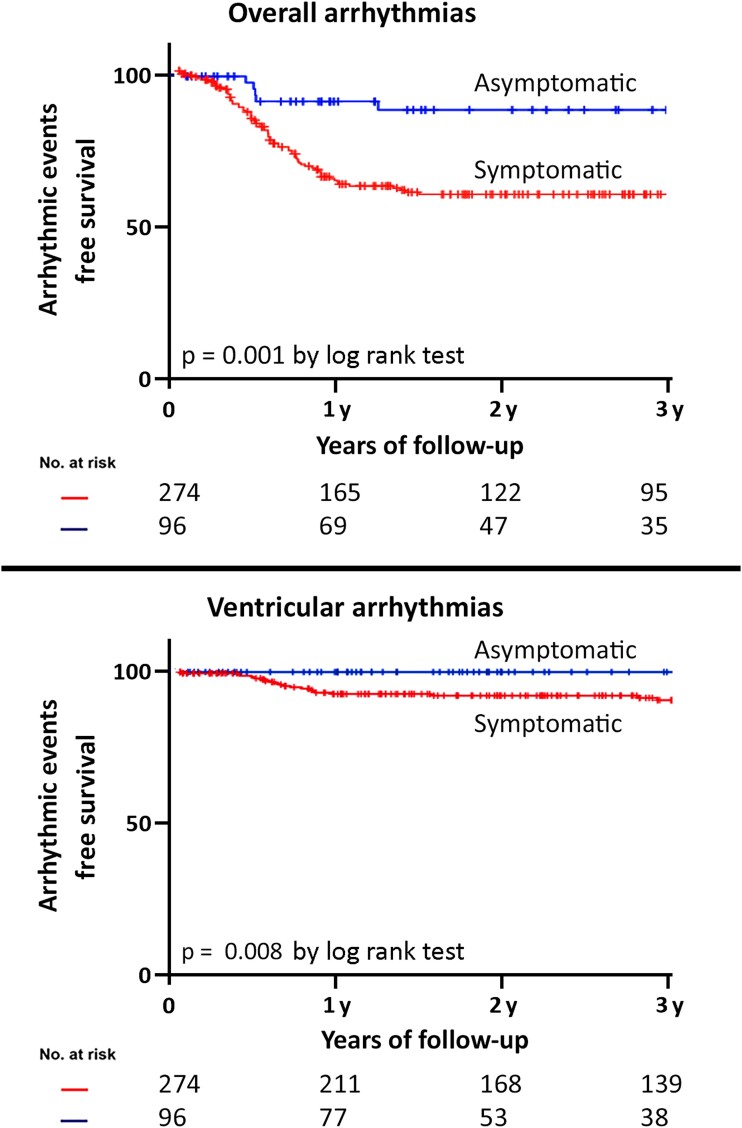
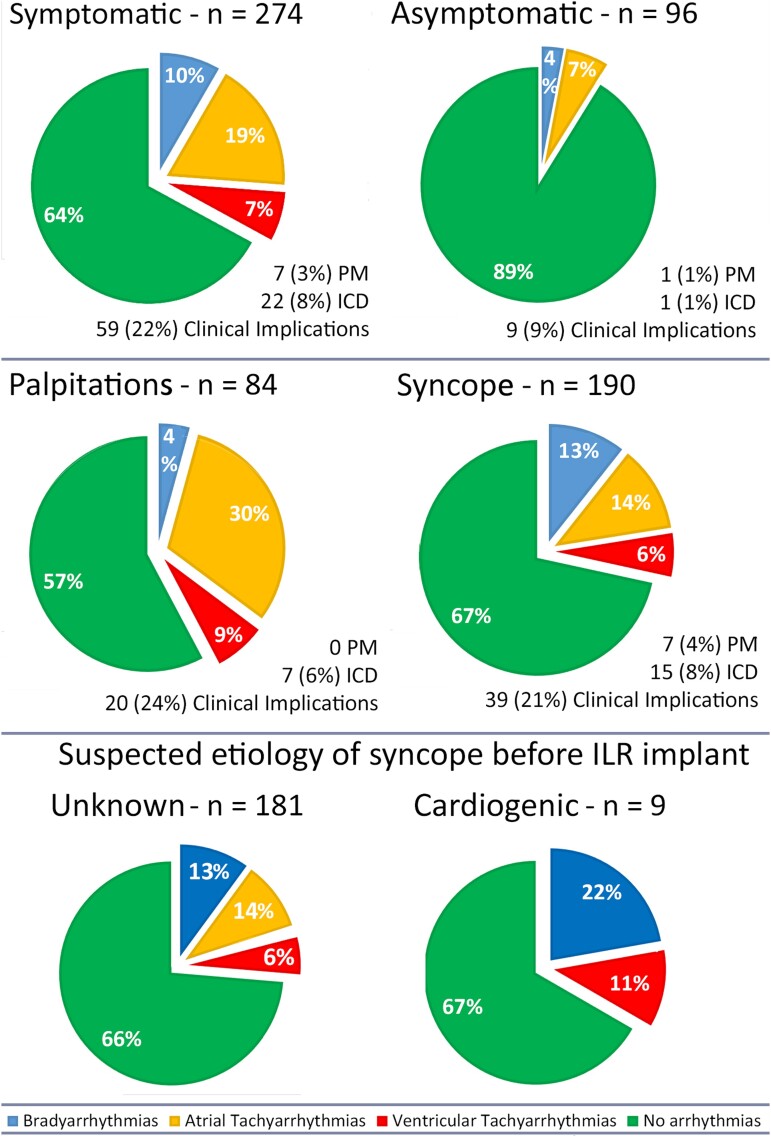
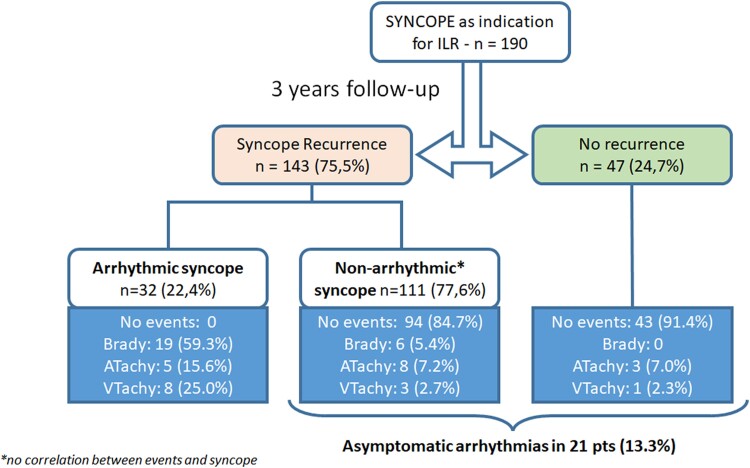
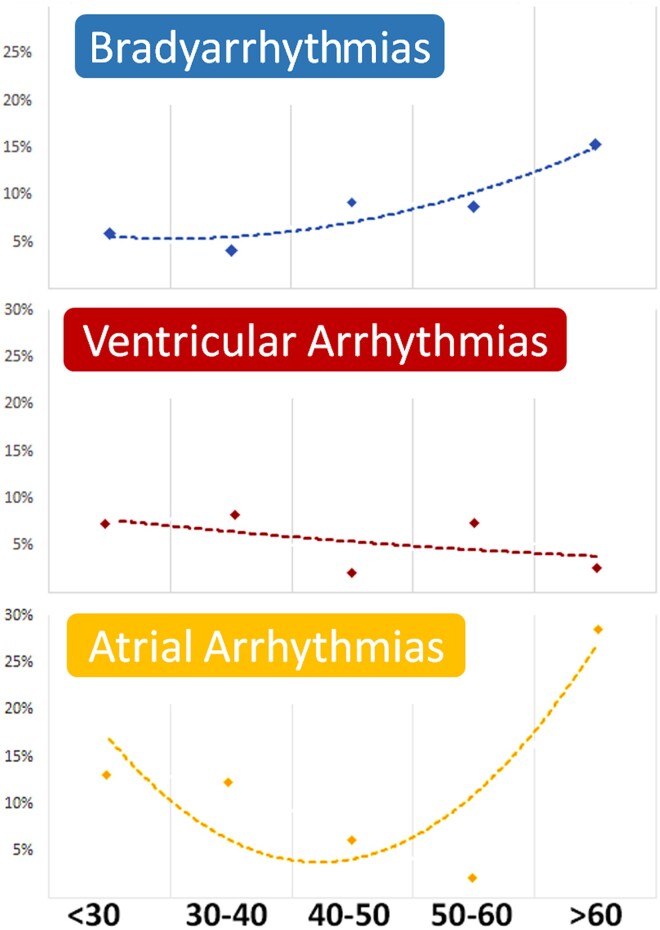
Results: During follow-up, an arrhythmic event was recorded in 30.7% of symptomatic patients [18.6% atrial arrhythmias (AAs), 10.2% bradyarrhythmias (BAs), and 7.3% ventricular arrhythmias (VAs)]. In patients with recurrent syncope, the aetiology was arrhythmic in 22.4% (59.3% BAs, 25.0% VAs, and 15.6% AAs). The ILR led to drug therapy initiation in 11.4%, ablation procedure in 10.9%, implantation of a pacemaker in 2.5%, and a cardioverter-defibrillator in 8%. At multivariate analysis, the presence of symptoms [hazard ratio (HR) 2.5, P = .001] and age >50 years (HR 1.7, P = .016) were independent predictors of arrhythmic events, while inducibility of ventricular fibrillation at the electrophysiological study (HR 9.0, P < .001) was a predictor of VAs.
Conclusions: ILR detects arrhythmic events in nearly 30% of symptomatic BrS patients, leading to appropriate therapy in 70% of them. The most commonly detected arrhythmias are AAs and BAs, while VAs are detected only in 7% of cases. Symptom status can be used to guide ILR implantation.
Keywords: Atrial arrhythmias; Brady-arrhythmias; Brugada syndrome; Loop recorder; Rhythm monitoring; Sudden cardiac death; Syncope; Ventricular arrhythmias.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Priori SG, Wilde AA, Horie M, Cho Y, Behr ER, Berul C, et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013. Heart Rhythm 2013;10:1932–63. 10.1016/j.hrthm.2013.05.014 - DOI - PubMed
