

Healthcare Burden and Resource Utilization After Pediatric Acute Respiratory Distress Syndrome: A Secondary Analysis of the Collaborative Pediatric Critical Care Research Network Acute Respiratory Distress Syndrome Study
- PMID: 38445974
- PMCID: PMC11178270
- DOI: 10.1097/PCC.0000000000003476
Healthcare Burden and Resource Utilization After Pediatric Acute Respiratory Distress Syndrome: A Secondary Analysis of the Collaborative Pediatric Critical Care Research Network Acute Respiratory Distress Syndrome Study
Abstract
Objectives: To describe family healthcare burden and health resource utilization in pediatric survivors of acute respiratory distress syndrome (ARDS) at 3 and 9 months.
Design: Secondary analysis of a prospective multisite cohort study.
Setting: Eight academic PICUs in the United States (2019-2020).
Patients: Critically ill children with ARDS and follow-up survey data collected at 3 and/or 9 months after the event.
Interventions: None.
Methods and measurement: We evaluated family healthcare burden, a measure of healthcare provided by families at home, and child health resource use including medication use and emergency department (ED) and hospital readmissions during the initial 3- and 9-month post-ARDS using proxy-report. Using multivariable logistic regression, we evaluated patient characteristics associated with family healthcare burden at 3 months.
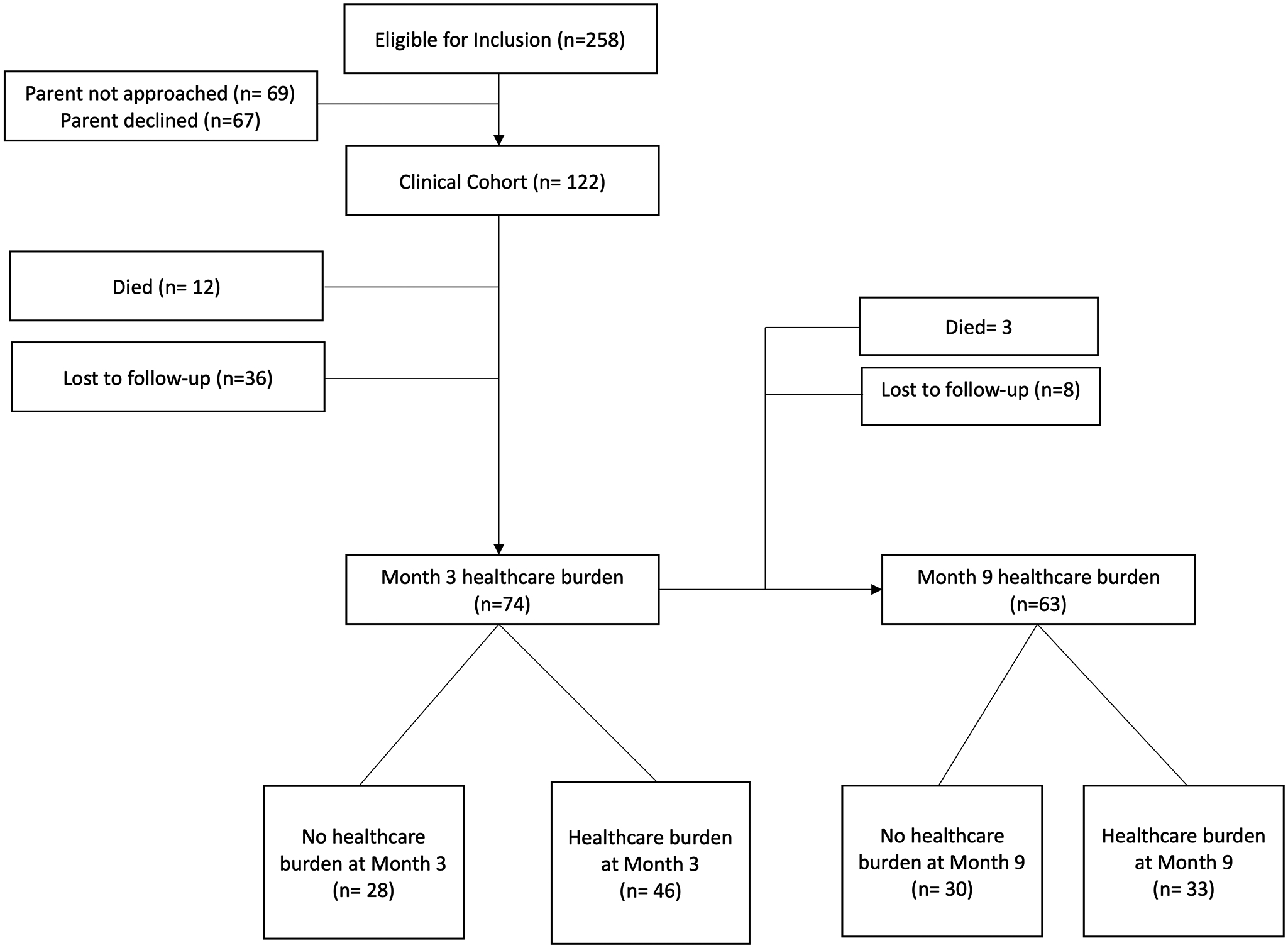
Main results: Of 109 eligible patients, 74 (68%) and 63 patients (58%) had follow-up at 3- and 9-month post-ARDS. At 3 months, 46 families (62%) reported healthcare burden including (22%) with unmet care coordination needs. At 9 months, 33 families (52%) reported healthcare burden including 10 families (16%) with unmet care coordination needs. At month 3, 61 patients (82%) required prescription medications, 13 patients (18%) had ED visits and 16 patients (22%) required hospital readmission. At month 9, 41 patients (65%) required prescription medications, 19 patients (30%) had ED visits, and 16 (25%) required hospital readmission were reported. Medication use was associated with family healthcare burden at both 3 and 9 months. In a multivariable analysis, preillness functional status and chronic conditions were associated with healthcare burden at month 3 but illness characteristics were not.
Conclusions: Pediatric ARDS survivors report high rates of healthcare burden and health resource utilization at 3- and 9-month post-ARDS. Future studies should assess the impact of improved care coordination to simplify care (e.g., medication management) and improve family burden.
Copyright © 2024 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Ames’ institution received funding from the Collaborative Pediatric Critical Care Research Network Sites (U01HD049934) and the National Institute for Child Health and Human Development (NICHD). Drs. Maddux, Fink, Meert, Zinter, Mourani, Carcillo, Carpenter, Pollack, and Sapru received support for article research from the National Institutes of Health (NIH). Dr. Maddux’s institution received funding from the NICHD (K23HD096018) and the Francis Family Foundation. Dr. Fink’s institution received funding from the Neurocritical Care Society and the American Board of Pediatrics. Drs. Fink, Meert, Mourani, Pollack, and Sapru’s institutions received funding from the NIH. Dr. Carcillo’s institution received funding from the National Institute of General Medical Sciences. Drs. Carcillo and Carpenter’s institutions received funding from the NICHD. The remaining authors have disclosed that they do not have any potential conflicts of interest.
References
-
- Shein SL, Maddux AB, Klein MJ, et al. : Epidemiology and Outcomes of Critically Ill Children at Risk for Pediatric Acute Respiratory Distress Syndrome: A Pediatric Acute Respiratory Distress Syndrome Incidence and Epidemiology Study. Crit Care Med 2021 - PubMed
-
- Yagiela LM, Barbaro RP, Quasney MW, et al. : Outcomes and Patterns of Healthcare Utilization After Hospitalization for Pediatric Critical Illness Due to Respiratory Failure. Pediatr Crit Care Med 2019; 20:120–127 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
